
临床荟萃 ›› 2025, Vol. 40 ›› Issue (1): 21-28.doi: 10.3969/j.issn.1004-583X.2025.01.003
刘金华1( ), 王春梅1, 王莹2, 陈凯1
), 王春梅1, 王莹2, 陈凯1
收稿日期:2024-09-28
出版日期:2025-01-20
发布日期:2025-01-17
通讯作者:
刘金华,Email:1067479381@qq.com基金资助:
Liu Jinhua1(), Wang Chunmei1, Wang Ying2, Chen Kai1
Received:2024-09-28
Online:2025-01-20
Published:2025-01-17
Contact:
Liu Jinhua,Email:1067479381@qq.com摘要:
目的 评价老年营养风险指数(GNRI)对老年急性缺血性卒中(acute ischemic stroke,AIS)阿替普酶静脉溶栓治疗患者短期转归的预测价值。方法 对天津市北辰医院自2021年7月-2024年1月进行阿替普酶静脉溶栓的773例老年AIS患者进行回顾性研究,根据其临床数据计算GNRI,并对其营养状态进行评价。应用改良的Rankin (mRS)评分对患者转归进行评估,其中转归不良组(mRS评分>2分)575例,转归良好组 (mRS评分≤2分) 198例。对GNRI与短期转归的关系进行logistic回归分析。结果 转归不良组GNRI明显低于转归良好组[90.106(84.622, 98.141) vs 90.722(82.239, 100.055), P<0.01]。多因素logistic回归结果表明:年龄、入院美国国立卫生研究院卒中量表(NIHSS)评分、心源性栓塞型(TOAST病因分型)、出血转化、体质量指数和低GNRI是短期转归不良的独立影响因子(P<0.01)。GNRI预测老年AIS患者静脉溶栓预后的ROC曲线下区域面积为0.876(95%CI: 0.845~0.907)。结论 GNRI是老年AIS患者营养不良与静脉溶栓后转归不良的独立风险因素并且GNRI可以作为一个重要的指标来评估老年AIS患者的免疫营养状况。
中图分类号:
刘金华, 王春梅, 王莹, 陈凯. 老年营养风险指数对老年急性脑梗死患者静脉溶栓短期转归的预测价值[J]. 临床荟萃, 2025, 40(1): 21-28.
Liu Jinhua, Wang Chunmei, Wang Ying, Chen Kai. The potential of geriatric nutritional risk index in predicting the short-term outcome of intravenous thrombolysis in elderly individuals with acute cerebral infarction[J]. Clinical Focus, 2025, 40(1): 21-28.
| 组别 | 例数 | 性别[例(%)] | 吸烟 [例(%)] | 饮酒 [例(%)] | 年龄 (年) | BMI (kg/m2) | 高血压 [例(%)] | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | ||||||||||||||
| 转归良好组 | 575 | 263(45.7) | 312(54.3) | 127(22.1) | 109(19.0) | 69.00±8.59 | 28.06±2.59 | 486(84.5) | |||||||
| 转归不良组 | 198 | 86(43.4) | 112(56.6) | 36(18.2) | 37(18.7) | 75.14±4.63 | 25.78±3.62 | 164(82.8) | |||||||
| 0.316 | 1.350 | 2.174 | 9.570 | 9.565 | 0.316 | ||||||||||
| 0.574 | 0.245 | 0.337 | <0.001 | <0.001 | 0.574 | ||||||||||
| 组别 | 糖尿病 [例(%)] | 脑卒中/TIA [例(%)] | 冠状动脉疾病 [例(%)] | 心房颤动 [例(%)] | SAO [例(%)] | LAA [例(%)] | CE [例(%)] | UND [例(%)] | |||||||
| 转归良好组 | 202(35.1) | 109(19.0) | 155(27.0) | 51(8.9) | 222(38.6) | 210(36.5) | 112(19.5) | 31(5.4) | |||||||
| 转归不良组 | 73(36.9) | 42(21.2) | 57(28.8) | 20(10.1) | 51(25.8) | 92(46.5) | 40(20.2) | 15(7.6) | |||||||
| χ2值 | 0.194 | 0.477 | 0.248 | 0.268 | 11.835 | ||||||||||
| 0.659 | 0.490 | 0.618 | 0.605 | 0.008 | |||||||||||
表1 2组一般资料比较
Tab.1 General information between the two groups
| 组别 | 例数 | 性别[例(%)] | 吸烟 [例(%)] | 饮酒 [例(%)] | 年龄 (年) | BMI (kg/m2) | 高血压 [例(%)] | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 男 | 女 | ||||||||||||||
| 转归良好组 | 575 | 263(45.7) | 312(54.3) | 127(22.1) | 109(19.0) | 69.00±8.59 | 28.06±2.59 | 486(84.5) | |||||||
| 转归不良组 | 198 | 86(43.4) | 112(56.6) | 36(18.2) | 37(18.7) | 75.14±4.63 | 25.78±3.62 | 164(82.8) | |||||||
| 0.316 | 1.350 | 2.174 | 9.570 | 9.565 | 0.316 | ||||||||||
| 0.574 | 0.245 | 0.337 | <0.001 | <0.001 | 0.574 | ||||||||||
| 组别 | 糖尿病 [例(%)] | 脑卒中/TIA [例(%)] | 冠状动脉疾病 [例(%)] | 心房颤动 [例(%)] | SAO [例(%)] | LAA [例(%)] | CE [例(%)] | UND [例(%)] | |||||||
| 转归良好组 | 202(35.1) | 109(19.0) | 155(27.0) | 51(8.9) | 222(38.6) | 210(36.5) | 112(19.5) | 31(5.4) | |||||||
| 转归不良组 | 73(36.9) | 42(21.2) | 57(28.8) | 20(10.1) | 51(25.8) | 92(46.5) | 40(20.2) | 15(7.6) | |||||||
| χ2值 | 0.194 | 0.477 | 0.248 | 0.268 | 11.835 | ||||||||||
| 0.659 | 0.490 | 0.618 | 0.605 | 0.008 | |||||||||||

图1 2组不同营养不良风险的发生率
Fig.1 Incidence of different malnutrition risks between the two groups
| 组别 | 例数 | NIHSS评分 (分) | 发病到溶栓 时间(h) | 出血转化 [例(%)] | 白细胞 (109/L) | 血红蛋白 (g/L) | 尿素氮 (mmol/L) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 转归良好组 | 575 | 4(2, 7) | 3.2(2.4, 3.8) | 12(2.1) | 7.7(5.8, 7.7) | 147.19±23.28 | 4.065(3.7, 5.53) | |||||
| 转归不良组 | 198 | 9(6, 12) | 3.7(2.5, 3.9) | 34(17.2) | 7.7(6.2, 7.7) | 142.69±26.19 | 4.59(3.7, 6.015) | |||||
| χ2/ | 9.952 | 3.516 | 59.882 | 0.734 | 2.272 | 2.426 | ||||||
| <0.001 | <0.001 | <0.001 | 0.463 | 0.023 | 0.015 | |||||||
| 组别 | 淋巴细胞 (109/L) | LDL-C (mmol/L) | 白蛋白 (g/L) | 肌酐 (μmol/L) | 空腹血糖 (mmol/L) | GNRI (分) | ||||||
| 转归良好组 | 2.148(1.898, 2.253) | 2.98(2.33, 3.70) | 39.4(36.3, 42.7) | 51(51, 64) | 5.2(4.8, 5.4) | 90.722(82.239, 100.055) | ||||||
| 转归不良组 | 2.148(2.067, 2.204) | 3.05(2.3, 3.81) | 39.9(35.7, 43) | 51(51, 62) | 5.2(5.2, 5.3) | 90.106(84.622, 98.141) | ||||||
| 1.247 | 0.648 | 0.708 | 1.272 | 1.384 | 6.108 | |||||||
| 0.212 | 0.517 | 0.479 | 0.203 | 0.166 | <0.001 | |||||||
表2 2组临床指标比较
Tab.2 Clinical indicators between the two groups
| 组别 | 例数 | NIHSS评分 (分) | 发病到溶栓 时间(h) | 出血转化 [例(%)] | 白细胞 (109/L) | 血红蛋白 (g/L) | 尿素氮 (mmol/L) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 转归良好组 | 575 | 4(2, 7) | 3.2(2.4, 3.8) | 12(2.1) | 7.7(5.8, 7.7) | 147.19±23.28 | 4.065(3.7, 5.53) | |||||
| 转归不良组 | 198 | 9(6, 12) | 3.7(2.5, 3.9) | 34(17.2) | 7.7(6.2, 7.7) | 142.69±26.19 | 4.59(3.7, 6.015) | |||||
| χ2/ | 9.952 | 3.516 | 59.882 | 0.734 | 2.272 | 2.426 | ||||||
| <0.001 | <0.001 | <0.001 | 0.463 | 0.023 | 0.015 | |||||||
| 组别 | 淋巴细胞 (109/L) | LDL-C (mmol/L) | 白蛋白 (g/L) | 肌酐 (μmol/L) | 空腹血糖 (mmol/L) | GNRI (分) | ||||||
| 转归良好组 | 2.148(1.898, 2.253) | 2.98(2.33, 3.70) | 39.4(36.3, 42.7) | 51(51, 64) | 5.2(4.8, 5.4) | 90.722(82.239, 100.055) | ||||||
| 转归不良组 | 2.148(2.067, 2.204) | 3.05(2.3, 3.81) | 39.9(35.7, 43) | 51(51, 62) | 5.2(5.2, 5.3) | 90.106(84.622, 98.141) | ||||||
| 1.247 | 0.648 | 0.708 | 1.272 | 1.384 | 6.108 | |||||||
| 0.212 | 0.517 | 0.479 | 0.203 | 0.166 | <0.001 | |||||||
| 项目 | 回归系数 | 标准误 | Wald χ2值 | 95% | |||
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 年龄 | 0.195 | 0.018 | 85.709 | <0.001 | 1.215 | 1.166 | 1.266 |
| 入院NIHSS评分 | 0.137 | 0.023 | 33.464 | <0.001 | 1.417 | 1.095 | 1.202 |
| TOAST病因分型 | |||||||
| SAO | - | 4.611 | 0.025 | - | - | ||
| LAA | 0.595 | 0.650 | 1.066 | 0.302 | 1.814 | 0.586 | 5.614 |
| CE | 1.214 | 0.639 | 4.696 | 0.030 | 3.367 | 1.123 | 10.096 |
| UND | 0.636 | 0.669 | 1.144 | 0.285 | 1.889 | 0.589 | 6.057 |
| 出血转化 | 0.216 | 0.057 | 34.831 | <0.001 | 1.241 | 1.155 | 1.333 |
| BMI | -2.328 | 0.048 | 18.922 | <0.001 | 0.097 | 0.034 | 0.278 |
| 低GNRI | 0.739 | 0.243 | 10.181 | 0.001 | 2.093 | 1.330 | 3.295 |
表3 AIS患者静脉溶栓短期转归危险因素的多因素logistic回归分析
Tab.3 Multivariate logistic regression analysis of risk factors for short-term outcomes of intravenous thrombolysis in AIS patients
| 项目 | 回归系数 | 标准误 | Wald χ2值 | 95% | |||
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 年龄 | 0.195 | 0.018 | 85.709 | <0.001 | 1.215 | 1.166 | 1.266 |
| 入院NIHSS评分 | 0.137 | 0.023 | 33.464 | <0.001 | 1.417 | 1.095 | 1.202 |
| TOAST病因分型 | |||||||
| SAO | - | 4.611 | 0.025 | - | - | ||
| LAA | 0.595 | 0.650 | 1.066 | 0.302 | 1.814 | 0.586 | 5.614 |
| CE | 1.214 | 0.639 | 4.696 | 0.030 | 3.367 | 1.123 | 10.096 |
| UND | 0.636 | 0.669 | 1.144 | 0.285 | 1.889 | 0.589 | 6.057 |
| 出血转化 | 0.216 | 0.057 | 34.831 | <0.001 | 1.241 | 1.155 | 1.333 |
| BMI | -2.328 | 0.048 | 18.922 | <0.001 | 0.097 | 0.034 | 0.278 |
| 低GNRI | 0.739 | 0.243 | 10.181 | 0.001 | 2.093 | 1.330 | 3.295 |
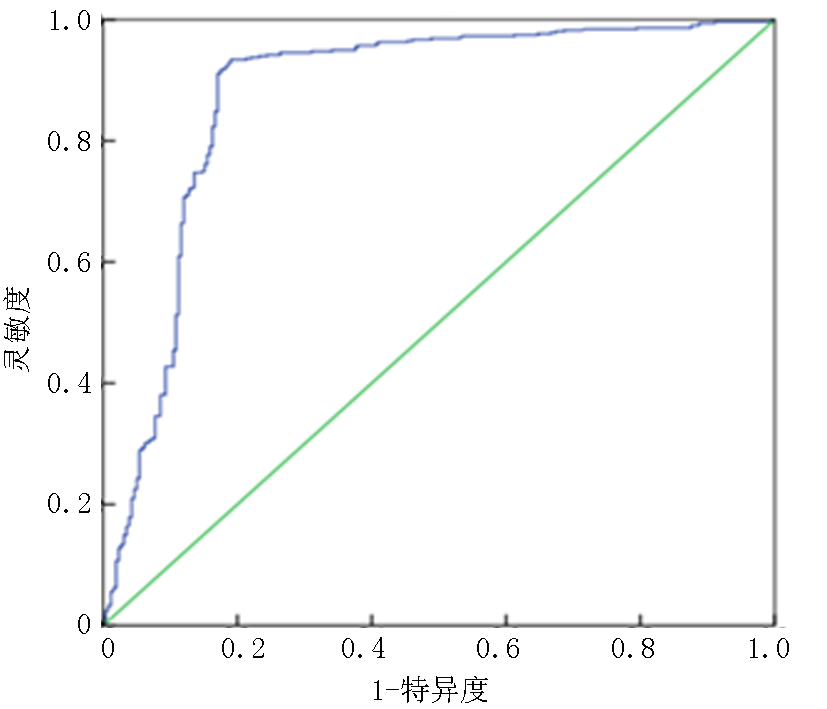
图2 GNRI预测老年AIS患者短期转归不良的ROC曲线
Fig.2 ROC curve of GNRI in predicting short-term poor outcomes in elderly AIS patients
| [1] |
GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990-2016: A systematic analysis for the global burden of disease study 2016[J]. Lancet Neurol, 2019, 18(5): 459-480.
doi: S1474-4422(18)30499-X pmid: 30879893 |
| [2] | Wang YJ, Li ZX, Gu HQ, et al. China stroke statistics: An update on the 2019 report from the National Center for Healthcare Quality Management in Neurological Diseases, China National Clinical Research Center for Neurological Diseases, the Chinese Stroke Association, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention and Institute for Global Neuroscience and Stroke Collaborations[J]. Stroke Vasc Neurol, 2022, 7(5): 415-450. |
| [3] | Wang W, Jiang B, Sun H, et al. Prevalence, incidence, and mortality of stroke in China: Results from a nationwide population-based survey of 480 687 adults[J]. Circulation, 2017, 135(8): 759-771. |
| [4] |
Dávalos A, Ricart W, Gonzalez-Huix F, et al. Effect of malnutrition after acute stroke on clinical outcome[J]. Stroke, 1996, 27(6): 1028-1032.
pmid: 8650709 |
| [5] |
Martineau J, Bauer JD, Isenring E, et al. Malnutrition determined by the patient-generated subjective global assessment is associated with poor outcomes in acute stroke patients[J]. Clin Nutr, 2005, 24(6): 1073-1077.
pmid: 16213064 |
| [6] |
Poor nutritional status on admission predicts poor outcomes after stroke: Observational data from the FOOD trial[J]. Stroke, 2003, 34(6): 1450-1456.
doi: 10.1161/01.STR.0000074037.49197.8C pmid: 12750536 |
| [7] |
Schuetz P, Fehr R, Baechli V, et al. Individualised nutritional support in medical inpatients at nutritional risk: A randomised clinical trial[J]. Lancet, 2019, 393(10188): 2312-2321.
doi: S0140-6736(18)32776-4 pmid: 31030981 |
| [8] |
Cederholm T, Bosaeus I, Barazzoni R, et al. Diagnostic criteria for malnutrition - an ESPEN consensus statement[J]. Clin Nutr, 2015, 34(3): 335-340.
doi: 10.1016/j.clnu.2015.03.001 pmid: 25799486 |
| [9] |
Jensen GL, Cederholm T, Correia M, et al. GLIM criteria for the diagnosis of malnutrition: A consensus report from the Global Clinical Nutrition Community[J]. JPEN J Parenter Enteral Nutr, 2019, 43(1): 32-40.
doi: 10.1002/jpen.1440 pmid: 30175461 |
| [10] |
Bouillanne O, Morineau G, Dupont C, et al. Geriatric nutritional risk index: A new index for evaluating at-risk elderly medical patients[J]. Am J Clin Nutr, 2005, 82(4): 777-783.
doi: 10.1093/ajcn/82.4.777 pmid: 16210706 |
| [11] | 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9): 666-682. |
| [12] | 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性脑梗死后出血转化诊治共识2019[J]. 中华神经科杂志, 2019, 52(4): 252-265. |
| [13] |
Bamford JM, Sandercock PA, Warlow CP, et al. Interobserver agreement for the assessment of handicap in stroke patients[J]. Stroke, 1989, 20(6): 828.
doi: 10.1161/01.str.20.6.828 pmid: 2728057 |
| [14] |
Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in acute stroke treatment[J]. Stroke, 1993, 24(1): 35-41.
doi: 10.1161/01.str.24.1.35 pmid: 7678184 |
| [15] |
Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association task force on practice guidelines and the obesity society[J]. J Am Coll Cardiol, 2014, 63(25 Pt B): 2985-3023.
doi: 10.1016/j.jacc.2013.11.004 pmid: 24239920 |
| [16] | Zhang G, Pan Y, Zhang R, et al. Prevalence and prognostic significance of malnutrition risk in patients with acute ischemic stroke: Results from the Third China National Stroke Registry[J]. Stroke, 2022, 53(1): 111-119. |
| [17] |
Zhang M, Ye S, Huang X, et al. Comparing the prognostic significance of nutritional screening tools and ESPEN-DCM on 3-month and 12-month outcomes in stroke patients[J]. Clin Nutr, 2021, 40(5): 3346-3353.
doi: 10.1016/j.clnu.2020.11.001 pmid: 33221053 |
| [18] |
Nishioka S, Omagari K, Nishioka E, et al. Concurrent and predictive validity of the mini nutritional assessment short-form and the geriatric nutritional risk index in older stroke rehabilitation patients[J]. J Hum Nutr Diet, 2020, 33(1): 12-22.
doi: 10.1111/jhn.12699 pmid: 31435986 |
| [19] |
Chen N, Li Y, Fang J, et al. Risk factors for malnutrition in stroke patients: A meta-analysis[J]. Clin Nutr, 2019, 38(1): 127-135.
doi: S0261-5614(17)31434-6 pmid: 29310894 |
| [20] | Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 Update to the 2018 guidelines for the early management of acute ischemic stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association[J]. Stroke, 2019, 50(12): e344-e418. |
| [21] |
Burgos R, Bretón I, Cereda E, et al. ESPEN guideline clinical nutrition in neurology[J]. Clin Nutr, 2018, 37(1): 354-396.
doi: S0261-5614(17)30318-7 pmid: 29274834 |
| [22] | Dennis M, Lewis S, Cranswick G, et al. FOOD: A multicentre randomised trial evaluating feeding policies in patients admitted to hospital with a recent stroke[J]. Health Technol Assess, 2006, 10(2): iii-iv, ix-x, 1-120. |
| [23] | Gao J, Zhao Y, Du M, et al. Serum albumin levels and clinical outcomes among ischemic stroke patients treated with endovascular thrombectomy[J]. Neuropsychiatr Dis Treat, 2021, 17: 401-411. |
| [24] |
Löwhagen Hendén P, Rentzos A, Karlsson JE, et al. Hypotension during endovascular treatment of ischemic stroke is a risk factor for poor neurological outcome[J]. Stroke, 2015, 46(9): 2678-2680.
doi: 10.1161/STROKEAHA.115.009808 pmid: 26173727 |
| [25] | Park HP, Nimmagadda A, DeFazio RA, et al. Albumin therapy augments the effect of thrombolysis on local vascular dynamics in a rat model of arteriolar thrombosis: A two-photon laser-scanning microscopy study[J]. Stroke, 2008, 39(5): 1556-1562. |
| [26] |
Reinhart WH, Nagy C. Albumin affects erythrocyte aggregation and sedimentation[J]. Eur J Clin Invest, 1995, 25(7): 523-528.
pmid: 7556371 |
| [27] | Jickling GC, Liu D, Stamova B, et al. Hemorrhagic transformation after ischemic stroke in animals and humans[J]. J Cereb Blood Flow Metab, 2014, 34(2): 185-199. |
| [28] | Zoellner H, Höfler M, Beckmann R, et al. Serum albumin is a specific inhibitor of apoptosis in human endothelial cells[J]. J Cell Sci, 1996, 109(Pt 10): 2571-2580. |
| [29] |
Spinella R, Sawhney R, Jalan R. Albumin in chronic liver disease: Structure, functions and therapeutic implications[J]. Hepatol Int, 2016, 10(1): 124-132.
doi: 10.1007/s12072-015-9665-6 pmid: 26420218 |
| [30] |
Che R, Huang X, Zhao W, et al. Low serum albumin level as a predictor of hemorrhage transformation after intravenous thrombolysis in ischemic stroke patients[J]. Sci Rep, 2017, 7(1): 7776.
doi: 10.1038/s41598-017-06802-y pmid: 28798356 |
| [31] | Naito H, Hosomi N, Nezu T, et al. Prognostic role of the controlling nutritional status score in acute ischemic stroke among stroke subtypes[J]. J Neurol Sci, 2020, 416: 116984. |
| [32] |
Gensicke H, Zinkstok SM, Roos YB, et al. IV thrombolysis and renal function[J]. Neurology, 2013, 81(20): 1780-1788.
doi: 10.1212/01.wnl.0000435550.83200.9e pmid: 24122182 |
| [33] | Lussier G, Evans AJ, Houston I, et al. Compact arterial monitoring device use in resuscitative endovascular balloon occlusion of the aorta (REBOA): A simple validation study in swine[J]. Cureus, 2024, 16(10): e70789. |
| [1] | 徐玉萍, 沈滔. 乳脂球表皮生长因子8对缺血性脑卒中后认知功能障碍的预测价值[J]. 临床荟萃, 2024, 39(6): 524-530. |
| [2] | 刘秀颖, 崔凯歌, 刘丽莹, 吴艳凯, 于佳琪, 杨冀萍. 基于静息态功能磁共振成像探讨卒中后疲劳的中枢机制[J]. 临床荟萃, 2024, 39(5): 401-407. |
| [3] | 宋梦姣, 王睿琪, 曹灿, 程光森, 刘羽, 李忠亮, 杨建豪. 血尿酸与首次急性缺血性脑卒中患者TOAST分型及预后的相关性[J]. 临床荟萃, 2024, 39(3): 216-221. |
| [4] | 李雯琳, 张志. 心房颤动患者左心耳形态结构和功能与左心耳血栓及心源性卒中的关系研究进展[J]. 临床荟萃, 2024, 39(2): 168-171. |
| [5] | 任大斌, 周晨辉, 张立国. 缺血性脑卒中发病率不均衡原因探究和预防[J]. 临床荟萃, 2024, 39(12): 1119-1124. |
| [6] | 张琦, 孙增鑫, 赵越, 袁野, 秦小露, 吕红香, 尹昱, 张雅文. 经颅直流电刺激对脑卒中患者单侧忽略康复效果的影响: 网状meta分析[J]. 临床荟萃, 2024, 39(12): 1061-1072. |
| [7] | 史莎莎, 任昊天, 宋丽菲, 李佳妮, 周岩, 张雁. 重症脑卒中患者肠内营养后高血糖管理的最佳证据总结[J]. 临床荟萃, 2024, 39(11): 1000-1006. |
| [8] | 朱静, 黄灿. 饮食与复发性缺血性卒中二级预防的研究进展[J]. 临床荟萃, 2024, 39(11): 1040-1046. |
| [9] | 张学谦, 李阳, 徐国栋, 吕佩源. 卵圆孔未闭所致急性脑梗死患者人口学特征、临床及影像学等特征分析[J]. 临床荟萃, 2023, 38(6): 500-503. |
| [10] | 辛燕红, 郎桂艳, 陈子为, 王东玉. 中性粒细胞-淋巴细胞比值和血小板-淋巴细胞比值预测急性轻型缺血性脑卒中患者认知障碍的价值[J]. 临床荟萃, 2023, 38(6): 504-509. |
| [11] | 贺翔渝, 潘燕, 张小林. 血清脂蛋白相关磷脂酶A2水平与急性缺血性脑卒中病情及预后的关系[J]. 临床荟萃, 2023, 38(4): 315-318. |
| [12] | 贾阳娟, 韩凝, 郭慧, 李岩鹏, 李灿灿, 李建国. MMSE和MoCA对卒中后轻度血管性认知障碍早期筛查的价值[J]. 临床荟萃, 2023, 38(3): 221-226. |
| [13] | 姚美芬, 丁刚玉, 徐建华, 王国江. 重组组织型纤溶酶原激活剂治疗急性轻型缺血性脑卒中的有效性和安全性[J]. 临床荟萃, 2023, 38(3): 227-231. |
| [14] | 赵越, 张少华, 赵振彪, 闫彦宁, 孙增鑫, 王晓晗, 吕佩源, 尹昱. 右侧忽略患者眼动追踪技术评估及认知训练1例并文献复习[J]. 临床荟萃, 2023, 38(3): 268-272. |
| [15] | 马宏莉, 陆皓, 王丹, 焦海星, 李一珂, 李思雨, 吕静. 脑卒中患者残疾危险因素的meta分析[J]. 临床荟萃, 2023, 38(2): 111-116. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||