Clinical Focus ›› 2022, Vol. 37 ›› Issue (6): 504-509.doi: 10.3969/j.issn.1004-583X.2022.06.004
Previous Articles Next Articles
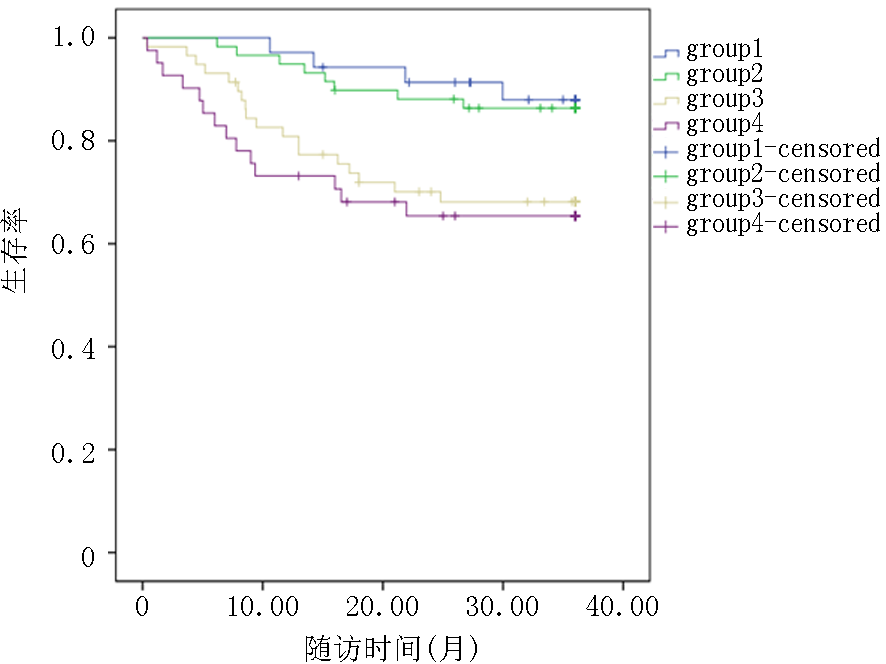
Clinical characteristics and long-term prognosis of initial patients with new onset different type of heart failure combined atrial fibrillation
Zhang Jingshui1a, Xu Yanan1b, Wang Jun1a, Yang Yi2, Jiang Haibing2, Tang Long1a, Wang Xianping1a, Shao Mingliang1a( )
)
- 1a. Department of Cardiology; b. Respiratory Medicine Department, the People's Hospital of Xuancheng City, Xuancheng 242000, China
2. Department of Cardiology, the Xinjiang Medical University Affiliated Hospital of Traditional Chinese Medicine, Urumqi 830011, China
-
Received:2022-02-09Online:2022-06-20Published:2022-08-05 -
Contact:Shao Mingliang E-mail:sml680328@163.com
CLC Number:
Cite this article
Zhang Jingshui, Xu Yanan, Wang Jun, Yang Yi, Jiang Haibing, Tang Long, Wang Xianping, Shao Mingliang. Clinical characteristics and long-term prognosis of initial patients with new onset different type of heart failure combined atrial fibrillation[J]. Clinical Focus, 2022, 37(6): 504-509.
share this article
Add to citation manager EndNote|Ris|BibTeX
URL: https://huicui.hebmu.edu.cn/EN/10.3969/j.issn.1004-583X.2022.06.004
| 项目 | Group 1(n=35) | Group 2(n=59) | Group 3(n=58) | Group 4(n=41) | F/Z/χ2值 | P值 |
|---|---|---|---|---|---|---|
| 男性[例(%)] | 18(51.4) | 35(59.3) | 22(37.9) | 26(63.4) | 8.008 | 0.046 |
| 年龄(岁) | 73.94±9.24 | 70.31±11.66 | 76.86±8.17 | 72.34±10.06 | 4.448 | 0.005 |
| 高血压[例(%)] | 20(57.1) | 25(42.4) | 26(44.8) | 20(48.8) | 2.112 | 0.549 |
| 糖尿病[例(%)] | 6(17.1) | 6(10.2) | 4(6.9) | 6(14.6) | 2.828 | 0.419 |
| 目前吸烟[例(%)] | 3(8.6) | 11(18.6) | 4(6.9) | 3(7.3) | 4.979 | 0.173 |
| 吸烟年数(年) | 33.33±5.77 | 30.00±17.32 | 30.79±17.04 | 29.00±24.75 | 0.081 | 0.969 |
| 每天吸烟数量(支) | 16.67±5.77 | 16.36±4.52 | 20.00±8.17 | 20.00±10.00 | 0.504 | 0.684 |
| BMI(kg/m2) | 21.71±4.06 | 21.52±3.30 | 21.30±3.19 | 21.76±3.29 | 0.183 | 0.908 |
| 冠心病[例(%)] | 10(28.6) | 14(23.7) | 7(12.1) | 6(14.6) | 5.219 | 0.156 |
| 既往PCI[例(%)] | 1(2.9) | 3(5.1) | 0(0.0) | 0(0.0) | 3.828 | 0.150 |
| NYHA分级[例(%)] | ||||||
| Ⅱ | 6(17.1) | 13(22.0) | 3(5.2) | 2(4.9) | ||
| Ⅲ | 20(57.1) | 34(57.6) | 38(65.5) | 20(48.8) | 16.320 | 0.012 |
| Ⅳ | 9(25.7) | 12(20.3) | 17(29.3) | 19(46.3) | ||
| 肌酐(μmol/L) | 96.20(71.80, 136.00) | 91.80(71.00, 112.90) | 86.10(68.95, 102.70) | 93.30(77.30, 112.05) | 2.776 | 0.427 |
| 尿素(mmol/L) | 9.08±4.26 | 8.22±3.78 | 7.86±4.02 | 8.52±4.67 | 0.645 | 0.587 |
| 尿酸(μmol/L) | 398.31±110.07 | 444.93±141.67 | 431.98±156.79 | 492.74±155.28 | 2.740 | 0.045 |
| 葡萄糖(mmol/L) | 5.75±1.72 | 5.29±1.47 | 5.45±1.77 | 5.38±1.71 | 0.557 | 0.644 |
| NT-proBNP (ng/L) | 7399.00 (3131.00, 13266.00) | 7688.00 (4629.00, 13954.00) | 4132.50 (2771.75, 7173.50) | 7188 (4714.50.00, 14705.00) | 18.899 | <0.01 |
| 左心室舒张末内径(mm) | 59.29±7.20 | 65.12±8.33 | 53.06±7.43 | 59.92±6.93 | 20.440 | <0.01 |
| LAD(mm) | 41.13±5.02 | 45.80±6.34 | 45.89±6.79 | 47.82±9.69 | 5.240 | 0.002 |
| LVEF (%) | 44(42, 48) | 31(27, 36) | 46(42, 48) | 32(28, 37) | 144.410 | <0.01 |
| CO | 6.10±1.77 | 6.18±2.07 | 4.97±1.83 | 5.92±1.85 | 1.074 | 0.365 |
| FS | 19.91±3.53 | 15.32±3.06 | 19.88±3.45 | 15.66±3.32 | 28.662 | <0.01 |
| CHA2DS2-VAS评分 | 3.23±0.77 | 3.00±1.17 | 3.29±1.04 | 3.34±1.13 | 1.096 | 0.352 |
| 用药[例(%)] | ||||||
| β受体阻滞剂 | 10(28.6) | 25(42.4) | 56(96.6) | 39(95.1) | 77.555 | <0.01 |
| ARB/ACEI | 20(57.1) | 25(42.4) | 26(44.8) | 20(48.8) | 2.112 | 0.549 |
| 利尿剂 | 22(62.9) | 57(96.6) | 47(81.0) | 41(100.0) | 32.575 | <0.01 |
| MACCEs[例(%)] | 4(11.4) | 8(13.6) | 18(31.0)*# | 14(34.1)*# | 10.667 | 0.014 |
| 项目 | Group 1(n=35) | Group 2(n=59) | Group 3(n=58) | Group 4(n=41) | F/Z/χ2值 | P值 |
|---|---|---|---|---|---|---|
| 男性[例(%)] | 18(51.4) | 35(59.3) | 22(37.9) | 26(63.4) | 8.008 | 0.046 |
| 年龄(岁) | 73.94±9.24 | 70.31±11.66 | 76.86±8.17 | 72.34±10.06 | 4.448 | 0.005 |
| 高血压[例(%)] | 20(57.1) | 25(42.4) | 26(44.8) | 20(48.8) | 2.112 | 0.549 |
| 糖尿病[例(%)] | 6(17.1) | 6(10.2) | 4(6.9) | 6(14.6) | 2.828 | 0.419 |
| 目前吸烟[例(%)] | 3(8.6) | 11(18.6) | 4(6.9) | 3(7.3) | 4.979 | 0.173 |
| 吸烟年数(年) | 33.33±5.77 | 30.00±17.32 | 30.79±17.04 | 29.00±24.75 | 0.081 | 0.969 |
| 每天吸烟数量(支) | 16.67±5.77 | 16.36±4.52 | 20.00±8.17 | 20.00±10.00 | 0.504 | 0.684 |
| BMI(kg/m2) | 21.71±4.06 | 21.52±3.30 | 21.30±3.19 | 21.76±3.29 | 0.183 | 0.908 |
| 冠心病[例(%)] | 10(28.6) | 14(23.7) | 7(12.1) | 6(14.6) | 5.219 | 0.156 |
| 既往PCI[例(%)] | 1(2.9) | 3(5.1) | 0(0.0) | 0(0.0) | 3.828 | 0.150 |
| NYHA分级[例(%)] | ||||||
| Ⅱ | 6(17.1) | 13(22.0) | 3(5.2) | 2(4.9) | ||
| Ⅲ | 20(57.1) | 34(57.6) | 38(65.5) | 20(48.8) | 16.320 | 0.012 |
| Ⅳ | 9(25.7) | 12(20.3) | 17(29.3) | 19(46.3) | ||
| 肌酐(μmol/L) | 96.20(71.80, 136.00) | 91.80(71.00, 112.90) | 86.10(68.95, 102.70) | 93.30(77.30, 112.05) | 2.776 | 0.427 |
| 尿素(mmol/L) | 9.08±4.26 | 8.22±3.78 | 7.86±4.02 | 8.52±4.67 | 0.645 | 0.587 |
| 尿酸(μmol/L) | 398.31±110.07 | 444.93±141.67 | 431.98±156.79 | 492.74±155.28 | 2.740 | 0.045 |
| 葡萄糖(mmol/L) | 5.75±1.72 | 5.29±1.47 | 5.45±1.77 | 5.38±1.71 | 0.557 | 0.644 |
| NT-proBNP (ng/L) | 7399.00 (3131.00, 13266.00) | 7688.00 (4629.00, 13954.00) | 4132.50 (2771.75, 7173.50) | 7188 (4714.50.00, 14705.00) | 18.899 | <0.01 |
| 左心室舒张末内径(mm) | 59.29±7.20 | 65.12±8.33 | 53.06±7.43 | 59.92±6.93 | 20.440 | <0.01 |
| LAD(mm) | 41.13±5.02 | 45.80±6.34 | 45.89±6.79 | 47.82±9.69 | 5.240 | 0.002 |
| LVEF (%) | 44(42, 48) | 31(27, 36) | 46(42, 48) | 32(28, 37) | 144.410 | <0.01 |
| CO | 6.10±1.77 | 6.18±2.07 | 4.97±1.83 | 5.92±1.85 | 1.074 | 0.365 |
| FS | 19.91±3.53 | 15.32±3.06 | 19.88±3.45 | 15.66±3.32 | 28.662 | <0.01 |
| CHA2DS2-VAS评分 | 3.23±0.77 | 3.00±1.17 | 3.29±1.04 | 3.34±1.13 | 1.096 | 0.352 |
| 用药[例(%)] | ||||||
| β受体阻滞剂 | 10(28.6) | 25(42.4) | 56(96.6) | 39(95.1) | 77.555 | <0.01 |
| ARB/ACEI | 20(57.1) | 25(42.4) | 26(44.8) | 20(48.8) | 2.112 | 0.549 |
| 利尿剂 | 22(62.9) | 57(96.6) | 47(81.0) | 41(100.0) | 32.575 | <0.01 |
| MACCEs[例(%)] | 4(11.4) | 8(13.6) | 18(31.0)*# | 14(34.1)*# | 10.667 | 0.014 |
| 指标 | 单因素分析 | 多因素分析 | |||||
|---|---|---|---|---|---|---|---|
| HR | 95%CI | P | HR | 95%CI | P | ||
| 性别(女) | 0.711 | 0.390-1.296 | 0.265 | ||||
| 年龄(岁) | 0.991 | 0.964-1.018 | 0.518 | ||||
| 高血压 | 1.033 | 0.572-1.866 | 0.915 | ||||
| 糖尿病 | 0.535 | 0.166-1.729 | 0.296 | ||||
| 目前吸烟 | 1.062 | 0.419-2.695 | 0.899 | ||||
| BMI | 1.013 | 0.931-1.103 | 0.758 | ||||
| 冠心病 | 1.090 | 0.524-2.268 | 0.817 | ||||
| 既往PCI | 0.989 | 0.136-7.185 | 0.991 | ||||
| NYHA分级 | 2.023 | 1.229-3.330 | 0.006 | 1.814 | 1.051-3.131 | 0.033 | |
| 肌酐(μmol/L) | 1.037 | 1.003-1.072 | 0.035 | 1.036 | 0.993-1.081 | 0.105 | |
| 尿酸(μmol/L) | 1.001 | 0.999-1.003 | 0.540 | ||||
| NT-proBNP (ng/L) | 1.036 | 1.001-1.072 | 0.046 | 1.076 | 1.033-1.120 | <0.01 | |
| LVEDD(mm) | 0.993 | 0.958-1.029 | 0.692 | ||||
| LAD(mm) | 1.009 | 0.968-1.052 | 0.667 | ||||
| CO | 0.892 | 0.651-1.222 | 0.476 | ||||
| FS | 1.085 | 1.008-1.169 | 0.030 | 1.073 | 0.988-1.165 | 0.096 | |
| CHA2DS2-VASc评分 | 1.705 | 1.268-2.293 | <0.01 | 1.375 | 1.022-1.851 | 0.036 | |
| β受体阻滞剂 | 1.641 | 0.829-3.248 | 0.155 | ||||
| ARB/ACEI | 1.033 | 0.572-1.866 | 0.915 | ||||
| 利尿剂 | 1.648 | 0.589-4.607 | 0.341 | ||||
| 临床分组 | |||||||
| Group2 vs Group1 | 1.207 | 0.363-4.007 | 0.759 | 1.910 | 0.536-6.810 | 0.318 | |
| Group3 vs Group1 | 3.199 | 1.082-9.457 | 0.035 | 5.023 | 1.565-16.118 | 0.007 | |
| Group4 vs Group1 | 3.818 | 1.256-11.603 | 0.018 | 5.822 | 1.699-19.955 | 0.005 | |
| 指标 | 单因素分析 | 多因素分析 | |||||
|---|---|---|---|---|---|---|---|
| HR | 95%CI | P | HR | 95%CI | P | ||
| 性别(女) | 0.711 | 0.390-1.296 | 0.265 | ||||
| 年龄(岁) | 0.991 | 0.964-1.018 | 0.518 | ||||
| 高血压 | 1.033 | 0.572-1.866 | 0.915 | ||||
| 糖尿病 | 0.535 | 0.166-1.729 | 0.296 | ||||
| 目前吸烟 | 1.062 | 0.419-2.695 | 0.899 | ||||
| BMI | 1.013 | 0.931-1.103 | 0.758 | ||||
| 冠心病 | 1.090 | 0.524-2.268 | 0.817 | ||||
| 既往PCI | 0.989 | 0.136-7.185 | 0.991 | ||||
| NYHA分级 | 2.023 | 1.229-3.330 | 0.006 | 1.814 | 1.051-3.131 | 0.033 | |
| 肌酐(μmol/L) | 1.037 | 1.003-1.072 | 0.035 | 1.036 | 0.993-1.081 | 0.105 | |
| 尿酸(μmol/L) | 1.001 | 0.999-1.003 | 0.540 | ||||
| NT-proBNP (ng/L) | 1.036 | 1.001-1.072 | 0.046 | 1.076 | 1.033-1.120 | <0.01 | |
| LVEDD(mm) | 0.993 | 0.958-1.029 | 0.692 | ||||
| LAD(mm) | 1.009 | 0.968-1.052 | 0.667 | ||||
| CO | 0.892 | 0.651-1.222 | 0.476 | ||||
| FS | 1.085 | 1.008-1.169 | 0.030 | 1.073 | 0.988-1.165 | 0.096 | |
| CHA2DS2-VASc评分 | 1.705 | 1.268-2.293 | <0.01 | 1.375 | 1.022-1.851 | 0.036 | |
| β受体阻滞剂 | 1.641 | 0.829-3.248 | 0.155 | ||||
| ARB/ACEI | 1.033 | 0.572-1.866 | 0.915 | ||||
| 利尿剂 | 1.648 | 0.589-4.607 | 0.341 | ||||
| 临床分组 | |||||||
| Group2 vs Group1 | 1.207 | 0.363-4.007 | 0.759 | 1.910 | 0.536-6.810 | 0.318 | |
| Group3 vs Group1 | 3.199 | 1.082-9.457 | 0.035 | 5.023 | 1.565-16.118 | 0.007 | |
| Group4 vs Group1 | 3.818 | 1.256-11.603 | 0.018 | 5.822 | 1.699-19.955 | 0.005 | |
| [1] | Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure[J]. Eur J Heart Fail, 2016, 18(8):2129. |
| [2] | 唐绪荣, 聂谦, 赵珏, 等. 射血分数中间值型心力衰竭的临床研究进展[J]. 心肺血管病杂志, 2020, 39(8): 1016-1019. |
| [3] | Maisel WH, Stevenson LW. Atrial fibrillation in heart failure: Epidemiology, pathophysiology, and rationale for therapy[J] .Am J Cardiol, 2003, 91(6A):2D-8D. |
| [4] |
Swedberg K, Olsson LG, Charlesworth A, et al. Prognostic relevance of atrial fibrillation in patients with chronic heart failure on long-term treatment with beta-blockers: Results from COMET[J] .Eur Heart J, 2005, 26(13): 1303-1308.
pmid: 15767288 |
| [5] |
Anter E, Jessup M, Callans DJ. Atrial fibrillation and heart failure: Treatment considerations for a dual epidemic[J] .Circulation, 2009, 119(18): 2516-2525.
doi: 10.1161/CIRCULATIONAHA.108.821306 pmid: 19433768 |
| [6] |
Mogensen UM, Jhund PS, Abraham WT, et al. Type of atrial fibrillation and outcomes in patients with heart failure and reduced ejection fraction[J] .J Am Coll Cardiol, 2017, 70(20): 2490-2500.
doi: S0735-1097(17)39778-4 pmid: 29145948 |
| [7] |
Dries DL, Exner DV, Gersh BJ, et al. Atrial fibrillation is associated with an increased risk for mortality and heart failure progression in patients with asymptomatic and symptomatic left ventricular systolic dysfunction: A retrospective analysis of the SOLVD trials. Studies of Left Ventric[J]. J Am Coll Cardiol, 1998, 32(3):695-703.
doi: 10.1016/s0735-1097(98)00297-6 pmid: 9741514 |
| [8] |
Ahmed MI, White M, Ekundayo OJ, et al. A history of atrial fibrillation and outcomes in chronic advanced systolic heart failure: A propensity-matched study[J]. Eur Heart J, 2009, 30(16):2029-2037.
doi: 10.1093/eurheartj/ehp222 URL |
| [9] |
Cheng M, Lu X, Huang J, et al. The prognostic significance of atrial fibrillation in heart failure with a preserved and reduced left ventricular function: Insights from a meta-analysis[J]. Eur J Heart Fail, 2014, 16(12):1317-1322.
doi: 10.1002/ejhf.187 pmid: 25371247 |
| [10] |
Romero R, Gaytán JM, Aguirre A, et al. The role of atrial fibrillation in the short-term outcomes of patients with acute heart failure[J] .Clin Res Cardiol, 2019, 108(6): 622-633.
doi: 10.1007/s00392-018-1389-x URL |
| [11] |
Hohendanner F, Heinzel FR, Blaschke F, et al. Pathophysiological and therapeutic implications in patients with atrial fibrillation and heart failure[J] .Heart Fail Rev, 2018, 23(1): 27-36.
doi: 10.1007/s10741-017-9657-9 pmid: 29038991 |
| [12] |
Lubitz SA, Moser C, Sullivan L, et al. Atrial fibrillation patterns and risks of subsequent stroke, heart failure, or death in the community[J] .J Am Heart Assoc, 2013, 2(5): e000126.
doi: 10.1161/JAHA.113.000126 URL |
| [13] |
Shotan A, Garty M, Blondhein DS, et al. Atrial fibrillation and long-term prognosis in patients hospitalized for heart failure: Results from heart failure survey in Israel (HFSIS)[J]. Eur Heart J, 2010, 31(3): 309-317.
doi: 10.1093/eurheartj/ehp422 URL |
| [14] | Cho Y, Oh IY, Park JJ, et al. Impact of successful restoration of sinus rhythm in patients with atrial fibrillation and acute heart failure: Results from the Korean Acute Heart Failure registry[J]. Cardiol J, 202229(3):472-480. |
| [15] |
Cunningham JW, Vaduganathan M, Claggett BL, et al. Effects of sacubitril/valsartan on N-terminal pro-B-type natriuretic peptide in heart failure with preserved ejection fraction[J]. JACC Heart Fail, 2020, 8(5):372-381.
doi: 10.1016/j.jchf.2020.03.002 URL |
| [16] |
Savarese G, Orsini N, Hage C, et al. Associations with and prognostic and discriminatory role of N-terminal pro-B-type natriuretic peptide in heart failure with preserved versus mid-range versus reduced ejection fraction[J]. J Card Fail, 2018, 24(6):365-374.
doi: 10.1016/j.cardfail.2018.03.010 URL |
| [17] | 蒋璐, 龚国彪, 康小兰, 等. 重组人脑利钠肽对严重心力衰竭患者心肌纤维化标志物水平的影响[J]. 疑难病杂志, 2020, 19(10):1005-1008. |
| [18] | Shuvy M, Zwas DR, Keren A, et al. Value of the CHA2DS2-VASc score for predicting outcome in patients with heart failure[J] .ESC Heart Fail, 2020, 7(5):2553-2560. |
| [19] |
Kajimoto K, Sato N. Investigators of the Acute Decompensated Heart Failure Syndromes (ATTEND) Registry.Sex differences in new york heart association functional classification and survival in acute heart failure patients with preserved or reduced ejection fraction[J] .Can J Cardiol, 2020, 36(1): 30-36.
doi: S0828-282X(19)31167-5 pmid: 31759787 |
| [20] |
Caraballo C, Desai NR, Mulder H, et al. Clinical implications of the new york heart association classification[J]. J Am Heart Assoc, 2019, 8(23): e014240.
doi: 10.1161/JAHA.119.014240 URL |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||