
临床荟萃 ›› 2023, Vol. 38 ›› Issue (9): 788-795.doi: 10.3969/j.issn.1004-583X.2023.09.003
李海1, 刘文虎2, 彭绍鹏2( ), 王飞3
), 王飞3
收稿日期:2023-02-20
出版日期:2023-09-20
发布日期:2023-11-21
通讯作者:
彭绍鹏, Email: 基金资助:
Li Hai1, Liu Wenhu2, Peng Shaopeng2(), Wang Fei3
Received:2023-02-20
Online:2023-09-20
Published:2023-11-21
Contact:
Peng Shaopeng,Email: 摘要:
目的 比较控制性阶梯式减压术与快速标准大骨瓣减压术治疗重度颅脑损伤的疗效。方法 计算机检索 PubMed、Embase、The Cochrane Library、Web of Science、万方医学网、CNKI、CBM和VIP数据库,查找自建库至2022年11月能查到的有关控制性阶梯式减压术和快速标准大骨瓣减压术治疗重度颅脑损伤疗效对比的相关文献,采用RevMan 5.4软件对符合条件的文献进行meta分析。结果 共纳入23篇文献,其中17篇是回顾性临床对照研究,6篇是随机对照试验,共计2141例患者,其中控制性阶梯式减压术患者1080例,快速标准大骨瓣减压术患者1061例。Meta分析结果显示,与快速标准大骨瓣减压术相比,控制性阶梯式减压术开始减压时间更早[
中图分类号:
李海, 刘文虎, 彭绍鹏, 王飞. 控制性阶梯式减压术对比快速标准大骨瓣减压术治疗重度颅脑损伤疗效的meta分析[J]. 临床荟萃, 2023, 38(9): 788-795.
Li Hai, Liu Wenhu, Peng Shaopeng, Wang Fei. Meta-analysis of the efficacy of controlled stepwise decompression versus rapid standard large bone-flap decompression on the treatment of severe craniocerebral injury[J]. Clinical Focus, 2023, 38(9): 788-795.
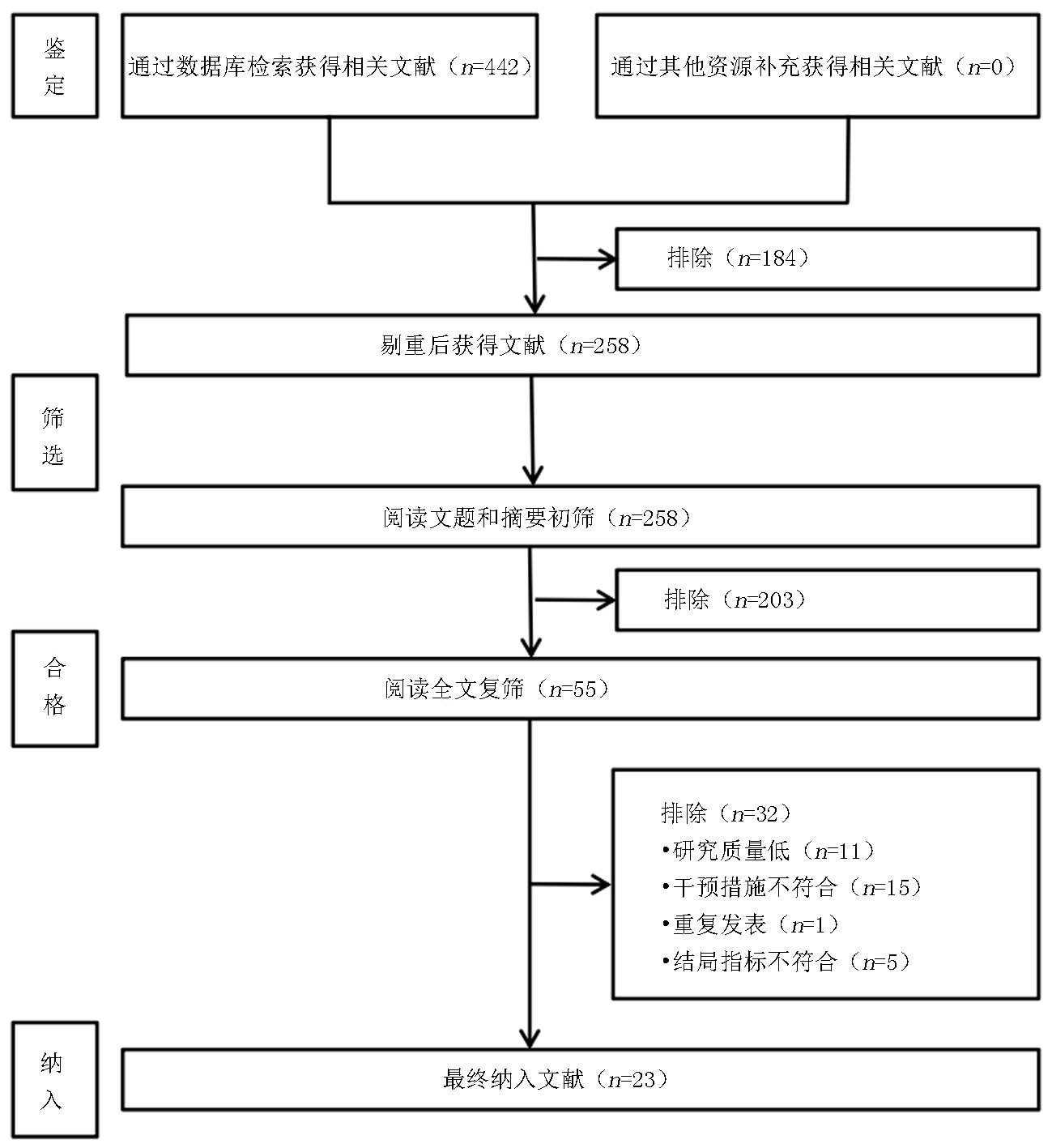
图1 文献检索及筛选流程图
Fig. 1 Flow chart of literature retrieval and screening
| 纳入研究 | 研究时间 | 研究类型 | 手术方式 | 例数 | 年龄(岁) | 男/女(例) |
|---|---|---|---|---|---|---|
| 李强2021[ | 2018.10-2020.10 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 40/40 | 43.5±2.4/42.8±2.8 | 26 14/25 15 |
| 张敏2021[ | 2018.01-2020.01 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 65/65 | 45.71±5.42/45.26±5.95 | 36 29/34 31 |
| 董陶2022[ | 2018.02-2020.03 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 41/41 | 44.42±7.01/43.76±6.99 | 24 17/25 16 |
| 许银才2022[ | 2014.02-2019.12 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 33/33 | 35.3±1.6/34.9±1.5 | 16 17/15 18 |
| 张清超2022[ | 2020.01-2020.12 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 60/60 | 45.3±12.86/45.4±13.71 | 37 23/39 21 |
| 蓝一帆2019[ | 2016.01-2018.10 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 43/43 | 44(28-60)/ 43(28-59) | 29 14/28 15 |
| 王星2018[ | 2010.01-2016.06 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 91/68 | 43.3±15.1/42.9±16.3 | 61 30/45 23 |
| 窦建胜2018[ | 2015.05-2017.05 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 48/45 | 46.2±6.9/45.8±6.5 | 38 10/34 11 |
| 王文刚2017[ | 2013.01-2016.10 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 40/40 | 45.10±5.21/46.12±5.41 | 25 15/26 14 |
| 谢树波2017[ | 2012.06-2016.06 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 60/56 | 43.52±11.03/43.28±10.36 | 40 20/35 21 |
| 付涛2017[ | 2013.08-2015.08 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 31/36 | 44.6±11.7/45.1±12.4 | 19 12/21 15 |
| 李军2015[ | 2011.01-2014.09 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 30/29 | 41.8±9.4/40.2±10.1 | 16 14/17 12 |
| 张继洲2019[ | 2016.08-2018.11 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 44/44 | 46.52±5.74/46.68±5.47 | 28 16/26 18 |
| 张永兵2019[ | 2015.07-2017.07 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 49/48 | 43.45±8.27/43.86±7.94 | 28 21/29 19 |
| 姜海涛2019[ | 2016.08-2017.08 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 32/32 | 51.04±3.41/51.08±3.45 | 16 16/17 15 |
| 赵永峰2019[ | 2014.01-2015.12 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 43/43 | 34.2±5.6/34.2±5.6 | —/— |
| 张毓2020[ | 2016.02-2019.02 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 58/64 | 39.5±10.4/37.8±12.5 | 42 16/47 17 |
| 靳腾龙2020[ | 2016.03-2019.03 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 44/44 | 45.58±6.33/45.61±6.27 | 24 20/26 18 |
| 焦锟2020[ | 2017.05-2018.10 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 49/51 | 42.34±5.01/43.15±4.67 | 32 17/30 21 |
| 周晓成2020[ | 2018.01-2019.01 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 42/42 | 41.95±10.86/40.98±10.37 | 27 15/26 16 |
| 孙阳2018[ | 2014.11-2015.12 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 34/34 | 33.04±3.58/35.21±3.17 | 25 9/23 11 |
| 王爱国2020[ | 2016.01-2019.12 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 53/53 | 43.87±6.22/44.46±6.69 | 31 22/29 24 |
| 孙翔宇2020[ | 2017.08-2019.08 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 50/50 | 42.53±2.05/42.25±1.88 | 25 25/21 29 |
表1 纳入研究的基本信息
Tab.1 Basic information of patients included in the study
| 纳入研究 | 研究时间 | 研究类型 | 手术方式 | 例数 | 年龄(岁) | 男/女(例) |
|---|---|---|---|---|---|---|
| 李强2021[ | 2018.10-2020.10 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 40/40 | 43.5±2.4/42.8±2.8 | 26 14/25 15 |
| 张敏2021[ | 2018.01-2020.01 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 65/65 | 45.71±5.42/45.26±5.95 | 36 29/34 31 |
| 董陶2022[ | 2018.02-2020.03 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 41/41 | 44.42±7.01/43.76±6.99 | 24 17/25 16 |
| 许银才2022[ | 2014.02-2019.12 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 33/33 | 35.3±1.6/34.9±1.5 | 16 17/15 18 |
| 张清超2022[ | 2020.01-2020.12 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 60/60 | 45.3±12.86/45.4±13.71 | 37 23/39 21 |
| 蓝一帆2019[ | 2016.01-2018.10 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 43/43 | 44(28-60)/ 43(28-59) | 29 14/28 15 |
| 王星2018[ | 2010.01-2016.06 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 91/68 | 43.3±15.1/42.9±16.3 | 61 30/45 23 |
| 窦建胜2018[ | 2015.05-2017.05 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 48/45 | 46.2±6.9/45.8±6.5 | 38 10/34 11 |
| 王文刚2017[ | 2013.01-2016.10 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 40/40 | 45.10±5.21/46.12±5.41 | 25 15/26 14 |
| 谢树波2017[ | 2012.06-2016.06 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 60/56 | 43.52±11.03/43.28±10.36 | 40 20/35 21 |
| 付涛2017[ | 2013.08-2015.08 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 31/36 | 44.6±11.7/45.1±12.4 | 19 12/21 15 |
| 李军2015[ | 2011.01-2014.09 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 30/29 | 41.8±9.4/40.2±10.1 | 16 14/17 12 |
| 张继洲2019[ | 2016.08-2018.11 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 44/44 | 46.52±5.74/46.68±5.47 | 28 16/26 18 |
| 张永兵2019[ | 2015.07-2017.07 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 49/48 | 43.45±8.27/43.86±7.94 | 28 21/29 19 |
| 姜海涛2019[ | 2016.08-2017.08 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 32/32 | 51.04±3.41/51.08±3.45 | 16 16/17 15 |
| 赵永峰2019[ | 2014.01-2015.12 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 43/43 | 34.2±5.6/34.2±5.6 | —/— |
| 张毓2020[ | 2016.02-2019.02 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 58/64 | 39.5±10.4/37.8±12.5 | 42 16/47 17 |
| 靳腾龙2020[ | 2016.03-2019.03 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 44/44 | 45.58±6.33/45.61±6.27 | 24 20/26 18 |
| 焦锟2020[ | 2017.05-2018.10 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 49/51 | 42.34±5.01/43.15±4.67 | 32 17/30 21 |
| 周晓成2020[ | 2018.01-2019.01 | 回顾性 | 控制性阶梯减压术/快速标准骨瓣减压术 | 42/42 | 41.95±10.86/40.98±10.37 | 27 15/26 16 |
| 孙阳2018[ | 2014.11-2015.12 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 34/34 | 33.04±3.58/35.21±3.17 | 25 9/23 11 |
| 王爱国2020[ | 2016.01-2019.12 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 53/53 | 43.87±6.22/44.46±6.69 | 31 22/29 24 |
| 孙翔宇2020[ | 2017.08-2019.08 | RCT | 控制性阶梯减压术/快速标准骨瓣减压术 | 50/50 | 42.53±2.05/42.25±1.88 | 25 25/21 29 |
| 纳入研究 | 研究人群 | 组间可比性 | 结果测量 | 评分 | |||||
|---|---|---|---|---|---|---|---|---|---|
| 暴露组 代表性 | 非暴露组 选择方法 | 暴露因素 确定方法 | 结局指标 | 结果评价 | 随访是否 够长 | 随访是否 充分 | |||
| 张敏2021[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 张清超2022[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 蓝一帆2019[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 王星2018[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 窦建胜2018[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 王文刚2017[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 谢树波2017[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 付涛2017[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 李军2015[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 张继洲2019[ | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| 张永兵2019[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 姜海涛2019[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 赵永峰2019[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 张毓2020[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 靳腾龙2020[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 焦锟2020[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 周晓成2020[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
表2 纳入队列研究NOS评分(分)
Tab.2 NOS scores of included cohort studies (scores)
| 纳入研究 | 研究人群 | 组间可比性 | 结果测量 | 评分 | |||||
|---|---|---|---|---|---|---|---|---|---|
| 暴露组 代表性 | 非暴露组 选择方法 | 暴露因素 确定方法 | 结局指标 | 结果评价 | 随访是否 够长 | 随访是否 充分 | |||
| 张敏2021[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 张清超2022[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 蓝一帆2019[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 王星2018[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 窦建胜2018[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 王文刚2017[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 谢树波2017[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 付涛2017[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 李军2015[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 张继洲2019[ | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| 张永兵2019[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 姜海涛2019[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 赵永峰2019[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 张毓2020[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 靳腾龙2020[ | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 8 |
| 焦锟2020[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| 周晓成2020[ | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
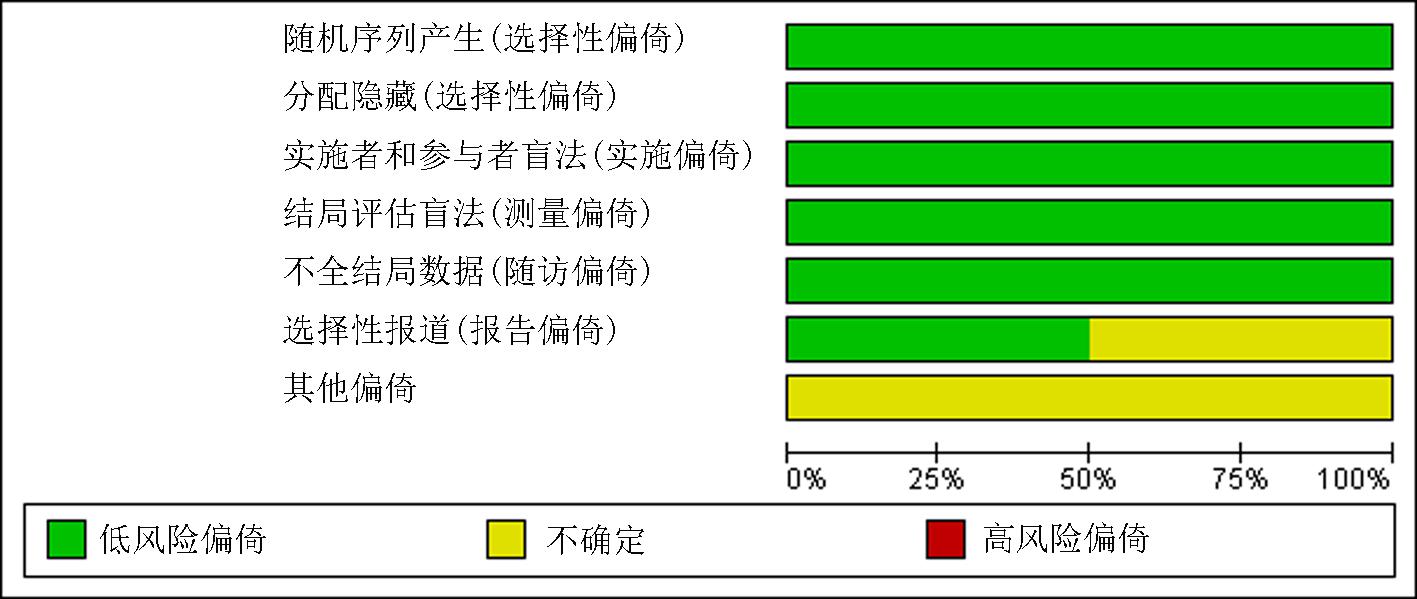
图2 RCT研究的偏倚风险图
Fig.2 Bias risk map for RCT studies
| 结局指标 | 文献 数量 | 样本量(例) | 效应模型 | 异质性 | 95% | ||||
|---|---|---|---|---|---|---|---|---|---|
| 控制性阶梯减压术 | 快速标准骨瓣减压术 | ||||||||
| 开始减压时间比较 | 3 | 184 | 161 | 随机 | 96% | <0.1 | -25.39 | (-30.96,-19.81) | <0.01 |
| 手术时间比较 | 10 | 510 | 492 | 随机 | 99% | <0.1 | -21.49 | (-34.22,-8.76) | <0.01 |
| 住院时间比较 | 3 | 118 | 118 | 随机 | 62% | 0.07 | -3.02 | (-3.70,-2.34) | <0.01 |
| 术中出血量比较 | 9 | 419 | 424 | 随机 | 98% | <0.1 | -23.82 | (-32.42,-15.22) | <0.01 |
| 减压术后第1天ICP | 5 | 232 | 231 | 随机 | 94% | <0.1 | -4.58 | (-6.03,-3.13) | <0.01 |
| 术后2周GCS评分 | 3 | 175 | 152 | 固定 | 0% | 0.91 | 1.94 | (1.31,2.56) | <0.01 |
表3 控制性阶梯式减压术与快速标准大骨瓣减压术术后部分结局指标的meta分析
Tab.3 Meta-analysis of some outcome indicators after controlled stepwise decompression and rapid standard large bone-flap decompression
| 结局指标 | 文献 数量 | 样本量(例) | 效应模型 | 异质性 | 95% | ||||
|---|---|---|---|---|---|---|---|---|---|
| 控制性阶梯减压术 | 快速标准骨瓣减压术 | ||||||||
| 开始减压时间比较 | 3 | 184 | 161 | 随机 | 96% | <0.1 | -25.39 | (-30.96,-19.81) | <0.01 |
| 手术时间比较 | 10 | 510 | 492 | 随机 | 99% | <0.1 | -21.49 | (-34.22,-8.76) | <0.01 |
| 住院时间比较 | 3 | 118 | 118 | 随机 | 62% | 0.07 | -3.02 | (-3.70,-2.34) | <0.01 |
| 术中出血量比较 | 9 | 419 | 424 | 随机 | 98% | <0.1 | -23.82 | (-32.42,-15.22) | <0.01 |
| 减压术后第1天ICP | 5 | 232 | 231 | 随机 | 94% | <0.1 | -4.58 | (-6.03,-3.13) | <0.01 |
| 术后2周GCS评分 | 3 | 175 | 152 | 固定 | 0% | 0.91 | 1.94 | (1.31,2.56) | <0.01 |
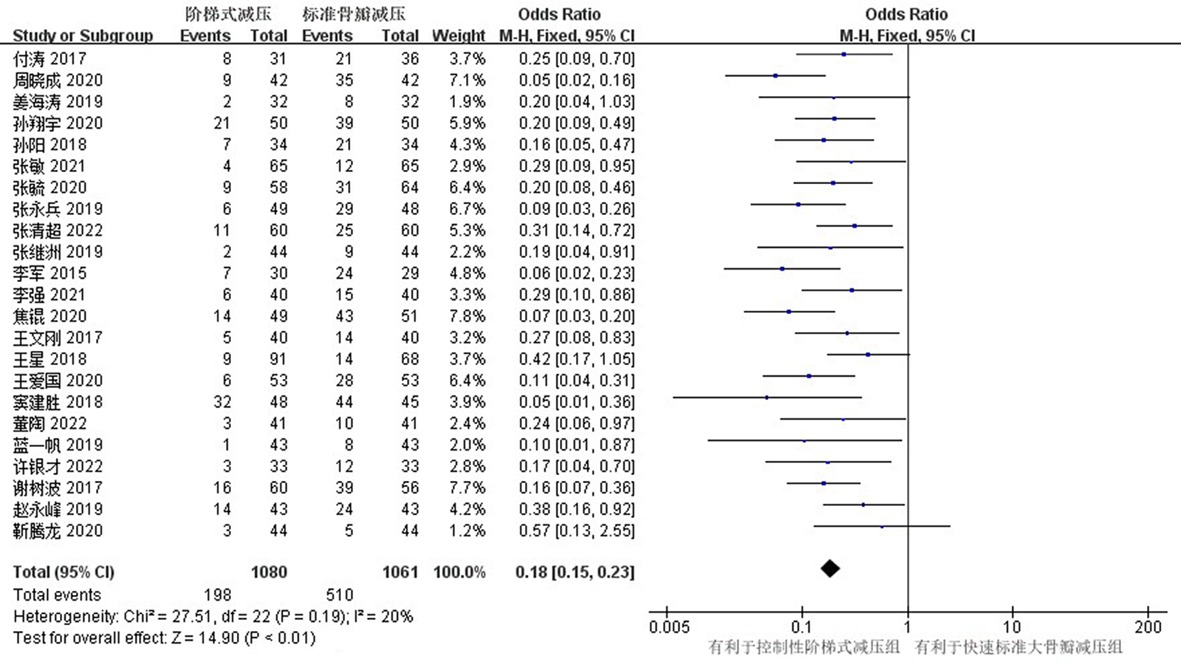
图3 控制性阶梯式减压术与快速标准大骨瓣减压术总并发症的meta分析
Fig.3 Meta-analysis of total complications of controlled stepwise decompression versus rapid standard large bone-flap decompression
| 结局指标 | 文献 数量 | 样本量(例) | 效应模型 | 异质性 | 95% | ||||
|---|---|---|---|---|---|---|---|---|---|
| 控制性阶梯减压术 | 快速标准骨瓣减压术 | ||||||||
| 术中脑膨出 | 23 | 1080 | 1061 | 固定 | 0% | 1 | 0.3 | (0.22,0.40) | <0.01 |
| 术后脑梗死 | 23 | 1080 | 1061 | 固定 | 0% | 0.93 | 0.34 | (0.24,0.49) | <0.01 |
| 迟发性血肿 | 23 | 1080 | 1061 | 固定 | 0% | 1 | 0.35 | (0.26,0.47) | <0.01 |
表4 控制性阶梯式减压术与快速标准大骨瓣减压术单一并发症的meta分析
Tab.4 Meta-analysis of single complication between controlled stepwise decompression and rapid standard large bone-flap decompression
| 结局指标 | 文献 数量 | 样本量(例) | 效应模型 | 异质性 | 95% | ||||
|---|---|---|---|---|---|---|---|---|---|
| 控制性阶梯减压术 | 快速标准骨瓣减压术 | ||||||||
| 术中脑膨出 | 23 | 1080 | 1061 | 固定 | 0% | 1 | 0.3 | (0.22,0.40) | <0.01 |
| 术后脑梗死 | 23 | 1080 | 1061 | 固定 | 0% | 0.93 | 0.34 | (0.24,0.49) | <0.01 |
| 迟发性血肿 | 23 | 1080 | 1061 | 固定 | 0% | 1 | 0.35 | (0.26,0.47) | <0.01 |
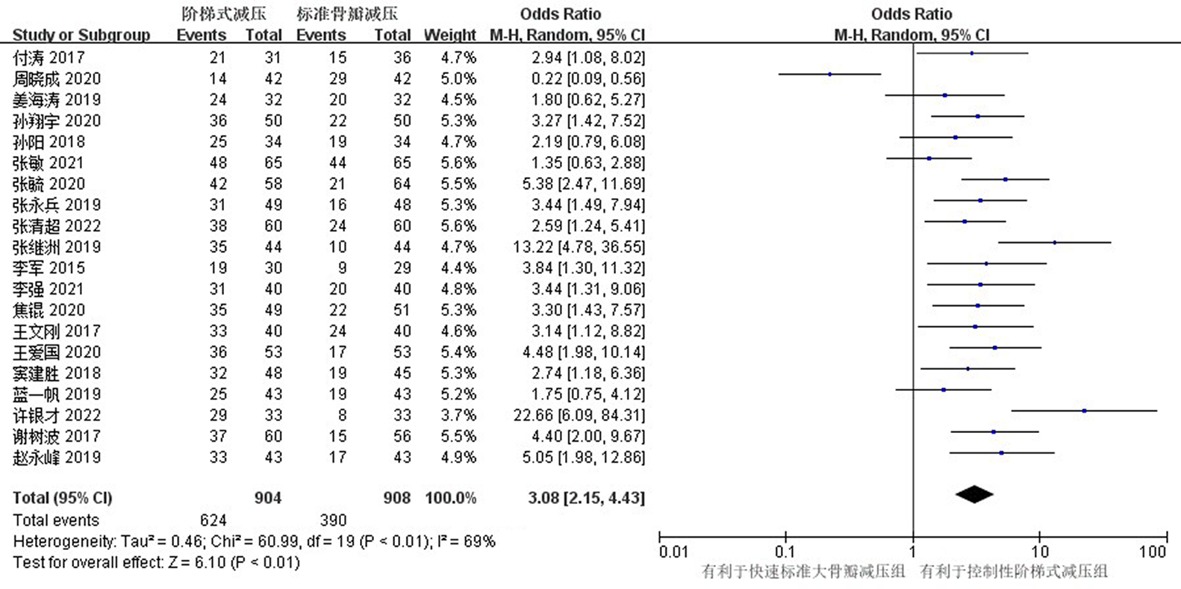
图4 控制性阶梯式减压术与快速标准大骨瓣减压术术后恢复良好的meta分析
Fig.4 Meta-analysis of good recovery after controlled stepwise decompression and rapid standard large bone-flap decompression
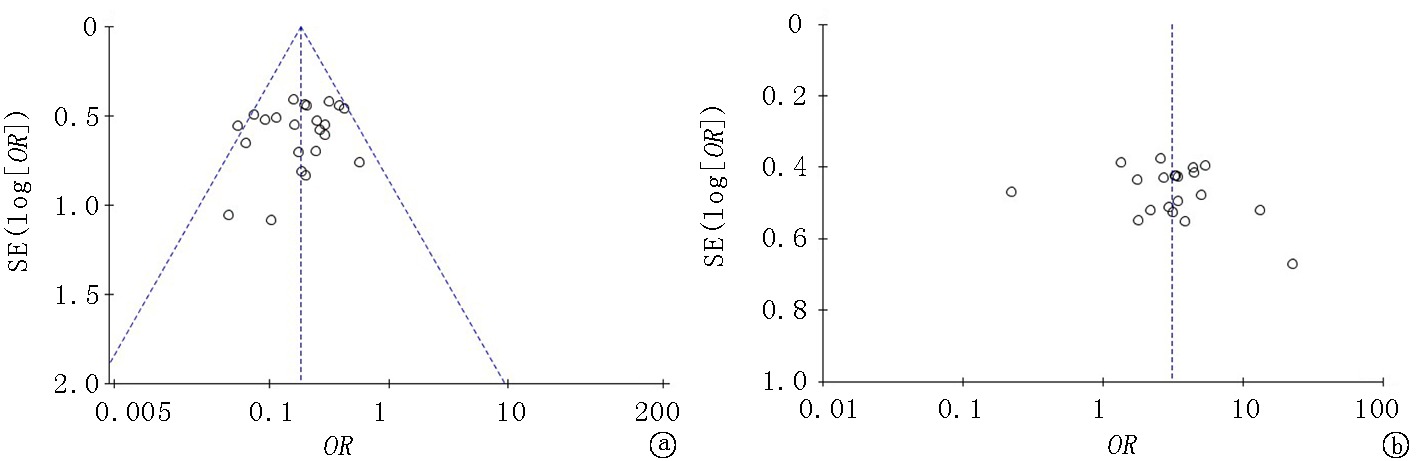
图5 控制性阶梯式减压术与快速标准大骨瓣减压术总并发症及预后恢复良好率的发表偏倚 a.总并发症;b.预后恢复良好
Fig.5 Publication bias of total complications and good prognosis between controlled stepwise decompression and rapid standard large bone-flap decompression a. total complications; b.good prognosis
| [1] |
Robinson CP. Moderate and severe traumatic brain injury[J]. Continuum (Minneap Minn), 2021, 27(5):1278-1300.
doi: 10.1212/CON.0000000000001036 pmid: 34618760 |
| [2] | Corral L, Javierre CF, Ventura JL, et al. Impact of non-neurological complications in severe traumatic brain injury outcome[J]. Crit Care, 2012, 16(2):R44. |
| [3] |
Jeffcote T, Weir T, Anstey J, et al. The impact of sedative choice on intracranial and systemic physiology in moderate to severe traumatic brain injury: A scoping review[J]. J Neurosurg Anesthesiol, 2023, 35(3):265-273.
doi: 10.1097/ANA.0000000000000836 URL |
| [4] | 高向前. 标准大骨瓣减压术治疗重型颅脑损伤的临床效果[J]. 河南外科学杂志, 2021, 27(3):115-116. |
| [5] | 李强. 分步控制性减压术治疗重型脑外伤的临床效果[J]. 当代医药论丛, 2021, 19(6):14-15. |
| [6] | 张敏, 徐珑, 马大程, 等. 控制性阶梯式减压应用于重型颅脑损伤手术患者的效果探讨[J]. 中外医疗, 2021, 40(8):66-68. |
| [7] | 董陶. 控制性阶梯式大骨瓣减压术与快速减压大骨瓣减压术治疗重型颅脑损伤的疗效对比[J]. 中国实用医药, 2022, 17(18):58-61. |
| [8] | 许银才. 阶梯式大骨瓣减压术在重型颅脑损伤的临床疗效[J]. 临床研究, 2022, 30(1):80-83. |
| [9] | 张清超, 查正江, 周和平. 控制性阶梯式减压术治疗重型颅脑损伤的效果分析[J]. 吉林医学, 2022, 43(6):1498-1500. |
| [10] | 曹崇秀. 重型颅脑外伤急性脑膨出预防策略及术后颅内感染高危因素对其预后的影响[J]. 中国医药科学, 2019, 9(22):218-220, 292. |
| [11] |
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses[J]. Eur J Epidemiol, 2010, 25(9):603-605.
doi: 10.1007/s10654-010-9491-z pmid: 20652370 |
| [12] | 蓝一帆. 比较常规大骨瓣减压术与控制性阶梯式减压术治疗重型颅脑损伤的效果[J]. 河南外科学杂志, 2019, 25(6):71-72. |
| [13] | 王星, 隗麟懿, 陈奎屹. 控制性阶梯式减压与传统大骨瓣减压术治疗重型颅脑损伤的对比分析[J]. 临床外科杂志, 2018, 26(10):773-776. |
| [14] | 窦建胜, 郑冀, 李君辉, 等. 分步控制性减压术治疗重型脑外伤的临床应用[J]. 临床和实验医学杂志, 2018, 17(10):1028-1030. |
| [15] | 王文刚, 贾亚宁. 控制性减压与大骨瓣减压术在重型颅脑损伤中的疗效和安全性比较[J]. 临床医学研究与实践, 2017, 2(21):74-75. |
| [16] | 谢树波, 蔡玮, 杨立业, 等. 阶梯减压式去骨瓣减压术对重型颅脑损伤术后转归的影响[J]. 中国临床神经外科杂志, 2017, 22(7):493-495. |
| [17] | 付涛. 标准大骨瓣减压术与阶梯式减压术治疗重型颅脑损伤的有效性和安全性对照[J]. 中国实用医刊, 2017, 44(13):49-52. |
| [18] | 李军, 管义祥, 缪永华, 等. 控制性减压在重型颅脑损伤开颅术中的应用[J]. 南通大学学报(医学版), 2015, 35(4):325-326. |
| [19] | 张继洲. 控制性阶梯式减压用于重型颅脑损伤手术的效果评价[J]. 临床研究, 2019, 27(10):18-20. |
| [20] | 张永兵. 控制性阶梯式颅内减压术治疗重型颅脑损伤疗效观察[J]. 医药论坛杂志, 2019, 40(5):68-70. |
| [21] | 姜海涛. 分步控制性减压术治疗重型脑外伤患者的临床疗效研究[J]. 中国医学创新, 2019, 16(22):141-144. |
| [22] | 赵永峰, 逯德胜, 贺志刚, 等. 分步控制性减压术治疗重型颅脑损伤的疗效评价[J]. 吉林医学, 2019, 40(8):1837-1838. |
| [23] | 张毓, 千超, 李峰, 等. 控制性阶梯式颅内减压术对重型颅脑损伤患者的有效性及NIHSS评分的影响[J]. 创伤外科杂志, 2020, 22(4):314-315. |
| [24] | 靳腾龙, 崔丙周, 王博, 等. 控制性阶梯式大骨瓣减压术与快速减压大骨瓣减压术治疗重型颅脑损伤患者的对比研究[J]. 实用中西医结合临床, 2020, 20(3):27-28, 89. |
| [25] | 焦锟, 马松, 王晗. 控制性减压与标准大骨瓣减压术治疗重症颅脑损伤的效果比较分析[J]. 哈尔滨医药, 2020, 40(4):313-315. |
| [26] | 周晓成. 阶梯减压式去骨瓣减压术对重型颅脑损伤患者的疗效[J]. 河南医学研究, 2020, 29(22):4079-4080. |
| [27] | 孙阳, 金薇薇, 高显峰, 等. 阶梯减压下去骨瓣减压术对重度颅脑损伤患者术后转归的影响[J]. 中华神经创伤外科电子杂志, 2018, 4(4):213-216. |
| [28] | 王爱国, 张小义. 控制性阶梯式减压术治疗重型颅脑损伤的效果观察[J]. 中国实用医刊, 2020, 47(20):43-45. |
| [29] | 孙翔宇. 分步控制性减压术治疗重型脑外伤的临床应用[J]. 系统医学, 2020, 5(18):111-113. |
| [30] |
Maas AI, Stocchetti N, Bullock R. Moderate and severe traumatic brain injury in adults[J]. Lancet Neurol, 2008, 7(8):728-741.
doi: 10.1016/S1474-4422(08)70164-9 pmid: 18635021 |
| [31] |
Kolias AG, Kirkpatrick PJ, Hutchinson PJ. Decompressive craniectomy: past, present and future[J]. Nat Rev Neurol, 2013, 9(7):405-415.
doi: 10.1038/nrneurol.2013.106 pmid: 23752906 |
| [32] | 张锋. 去骨瓣减压术在重型颅脑损伤中的应用进展[J]. 现代诊断与治疗, 2022, 33(9):1297-1299. |
| [33] |
Cooper DJ, Rosenfeld JV, Murray L, et al. Patient outcomes at twelve months after early decompressive craniectomy for diffuse traumatic brain injury in the randomized DECRA clinical trial[J]. J Neurotrauma, 2020, 37(5):810-816.
doi: 10.1089/neu.2019.6869 URL |
| [34] |
Giese H, Antritter J, Unterberg A, et al. Long-term results of neurological outcome, quality of life, and cosmetic outcome after cranioplastic surgery: A single center study of 202 patients[J]. Front Neurol, 2021, 12:702339.
doi: 10.3389/fneur.2021.702339 URL |
| [35] | 程勇, 秦加新, 戢翰升, 等. 颅脑损伤术中急性脑膨出的相关因素分析[J]. 中国临床神经外科杂志, 2016, 21(6):374-375. |
| [36] |
Timofeev I, Hutchinson PJ. Outcome after surgical decompression of severe traumatic brain injury[J]. Injury, 2006, 37(12):1125-1132.
doi: 10.1016/j.injury.2006.07.031 pmid: 17081545 |
| [37] |
Mitchell P, Tseng M, Mendelow AD. Decompressive craniectomy with lattice duraplasty[J]. Acta Neurochir (Wien), 2004, 146(2):159-160.
doi: 10.1007/s00701-003-0186-z URL |
| [38] | 杜春雷, 刘连松, 平海江, 等. 梯度减压防治颅脑创伤开颅术中恶性脑膨出[J]. 中华神经外科杂志, 2014, 30(3):260-262. |
| [39] |
Mork J, Mraček J, Štěpánek D, et al. Surgical complications of decompressive craniectomy in patients with head injury[J]. Rozhl Chir, 2020, 99(7):316-322.
doi: 10.33699/PIS.2020.99.7.316-322 pmid: 32972150 |
| [40] | 蒲建章, 苏群, 李力, 等. 重型颅脑损伤开颅术中急性脑膨出的防治[J]. 中国临床神经外科杂志, 2012, 17(1):15-17. |
| [41] | 赵鹤翔, 徐丁, 杨朝华. 有占位效应的重型颅脑损伤术后再次手术去骨瓣减压41例分析[J]. 创伤外科杂志, 2017, 19(5):379-381. |
| [42] | 林利刚, 林达, 林高钧, 等. 重型颅脑损伤术中脑膨出分析及处理[J]. 中国医师杂志, 2018, 20(3):437-439. |
| [1] | 龚财芳, 赵俊宇, 游川. 接纳与承诺疗法对癌症患者心理健康和生活质量影响的meta分析[J]. 临床荟萃, 2024, 39(2): 101-107. |
| [2] | 肖煌怡, 袁建坤, 严梓予, 曾雯姝, 鲁兰莫, 王峻. 认知干预对遗忘型轻度认知障碍老年患者干预效果的meta分析[J]. 临床荟萃, 2024, 39(1): 12-19. |
| [3] | 吕畅, 周利明. TNF-α-308基因多态性与胃癌易感相关性的meta分析[J]. 临床荟萃, 2023, 38(9): 779-787. |
| [4] | 侯有玲, 李奕, 关红玉, 罗红霞. 目标导向液体治疗在脑肿瘤切除术中应用效果的meta分析[J]. 临床荟萃, 2023, 38(8): 686-693. |
| [5] | 金家辉, 杨阳, 秦铜, 何雨欣, 苏美华. 补充益生菌对2型糖尿病患者糖代谢改善的meta分析[J]. 临床荟萃, 2023, 38(7): 581-587. |
| [6] | 肖王静, 李欣梦, 卢松玲, 孙雪华. 重复经颅磁刺激治疗中枢神经源性吞咽障碍疗效及安全性的meta分析[J]. 临床荟萃, 2023, 38(7): 588-599. |
| [7] | 尤奕, 高淑清, 徐浩. 肠内营养对食管癌患者术后临床结局影响的系统综述[J]. 临床荟萃, 2023, 38(6): 485-492. |
| [8] | 倪艺芸, 刘彬, 梁琪, 李晓凤. 白细胞介素6和C反应蛋白预测新型冠状病毒肺炎严重程度的meta分析[J]. 临床荟萃, 2023, 38(6): 493-499. |
| [9] | 沃拉孜汗·玛德尼亚提, 迪力夏提·图尔迪麦麦提, 李梦晨, 拜合提尼沙·吐尔地. 宏基因组二代测序技术在肺结核诊断中应用价值的meta分析[J]. 临床荟萃, 2023, 38(5): 389-398. |
| [10] | 赵哲, 穆培娟, 张冬. 恩度联合顺铂胸腔灌注治疗肺癌合并恶性胸腔积液疗效的meta分析[J]. 临床荟萃, 2023, 38(5): 399-404. |
| [11] | 马明福, 魏志国, 何铁英. 急性胰腺炎并发胰腺假性囊肿危险因素的meta分析[J]. 临床荟萃, 2023, 38(4): 293-301. |
| [12] | 曹宇萌, 张海燕, 刘立新. 非酒精性脂肪性肝病的病理改变与血清铁蛋白和血清铁含量变化关系的meta分析[J]. 临床荟萃, 2023, 38(3): 197-207. |
| [13] | 马宏莉, 陆皓, 王丹, 焦海星, 李一珂, 李思雨, 吕静. 脑卒中患者残疾危险因素的meta分析[J]. 临床荟萃, 2023, 38(2): 111-116. |
| [14] | 陶嘉楠, 李文茜, 马秀雯, 安琪, 王学红. HER-2在肝细胞癌中表达及临床意义的meta分析[J]. 临床荟萃, 2023, 38(12): 1067-1072. |
| [15] | 柯孟婷, 陈慰. 瑞舒伐他汀降压作用的meta分析[J]. 临床荟萃, 2023, 38(11): 965-971. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||