
临床荟萃 ›› 2022, Vol. 37 ›› Issue (3): 234-242.doi: 10.3969/j.issn.1004-583X.2022.03.007
高鹏丽, 陈丽丽, 田芬, 张嘉倩, 陈怿鹏, 亓晓菁, 邢广群( )
)
收稿日期:2021-09-12
出版日期:2022-03-20
发布日期:2022-04-02
通讯作者:
邢广群
E-mail:gqx99monash@163.com
基金资助:
Gao Pengli, Chen Lili, Tian Fen, Zhang Jiaqian, Chen Yipeng, Qi Xiaojing, Xing Guangqun()
Received:2021-09-12
Online:2022-03-20
Published:2022-04-02
Contact:
Xing Guangqun
E-mail:gqx99monash@163.com
摘要:
目的 探讨人体质量指数(body mass index, BMI)对IgA肾病(IgA nephropathy, IgAN)患者的临床病理及其预后的影响。方法 回顾性分析2013年2月至2021年5月在青岛大学附属医院就诊并经肾穿刺活检确诊为原发性IgAN的初治患者的临床病理资料及预后,终点事件为血肌酐翻倍和(或)进入终末期肾病(end-stage renal disease, ESRD)和(或)肾替代治疗和(或)死亡。根据患者接受肾活检时的BMI及WHO肥胖分类分组如下:低体重组(BMI<18.5 kg/m2)、正常体重组(18.5≤BMI<25.0 kg/m2)和超重肥胖组(BMI≥25.0 kg/m2)。比较各组临床病理资料、预后的差异。采用Kaplan-Meier生存曲线评估患者肾脏累计生存率,多因素Cox回归分析影响IgAN合并超重肥胖患者肾脏预后的危险因素。结果 共入选533例IgAN患者,其中低体重组19例(3.6%),正常体重组267例(50.1%),超重肥胖组247例(46.3%)。与低体重组、正常体重组比较,超重肥胖组的年龄、收缩压、舒张压、血管紧张素转换酶抑制剂(angiotensin-converting-enzyme inhibitors,ACEI)/血管紧张素Ⅱ 1型受体拮抗剂(angiotensin Ⅱ receptor type 1,ARB)使用占比、血红蛋白、24小时尿蛋白排泄量、甘油三酯、空腹血糖、血清补体C3、血清补体C4、尿酸较高,而高密度脂蛋白胆固醇(high-density lipoprotein cholesterol,HDL-C)、估算的肾小球滤过率(estimated glomerular filtration rate,eGFR)水平较低(均P<0.05)。正常体重组年龄、收缩压、舒张压、ACEI/ARB使用比例、尿酸高于低体重组,而eGFR低于低体重组(均P<0.05)。超重肥胖组和正常体重组的低密度脂蛋白胆固醇(low-density lipoprotein cholesterol,LDL-C)高于低体重组(均P<0.05)。与正常体重组比较,超重肥胖组的免疫球蛋白M水平较低,男性占比、C反应蛋白(C-reactive protein,CRP)水平较高(均P<0.05)。低体重组的中性粒细胞计数高于正常体重组(P<0.05)。光镜检查结果显示,超重肥胖组、正常体重组的血管损伤程度、炎细胞浸润程度高于低体重组(均P<0.05)。与正常体重组比较,超重肥胖组的系膜C3沉积减弱(P<0.05)。Kaplan-Meier生存曲线分析表明,正常体重组的肾脏累积生存率高于超重肥胖组(Log-rank检验,χ2=8.702,P=0.003),而超重肥胖组肾脏累积生存率高于低体重组(Log-rank检验,χ2=4.624,P=0.032)。3组的肾脏5年生存率分别为69.8%、75.6%、85.9%,正常体重组的5年肾脏生存率高于超重肥胖组(Log-rank检验,χ2=4.996,P=0.025),而超重肥胖组的5年生存率高于低体重组(Log-rank检验,χ2=5.764,P=0.016)。在IgAN合并超重肥胖患者中,多因素Cox回归分析结果提示,24小时尿蛋白排泄量、甘油三酯、血红蛋白是发生肾脏终点事件的独立危险因素。结论 IgAN合并超重肥胖患者临床表现较重,有着更重的血管损伤及炎细胞浸润,肾脏预后较差。应重视IgAN合并超重肥胖患者的治疗及随访过程中生活方式及体重的管理。
中图分类号:
高鹏丽, 陈丽丽, 田芬, 张嘉倩, 陈怿鹏, 亓晓菁, 邢广群. 体质量指数对IgA肾病患者临床病理及预后的影响[J]. 临床荟萃, 2022, 37(3): 234-242.
Gao Pengli, Chen Lili, Tian Fen, Zhang Jiaqian, Chen Yipeng, Qi Xiaojing, Xing Guangqun. Impact of body mass index in the clinicopathology and prognosis of patients with IgA nephropathy[J]. Clinical Focus, 2022, 37(3): 234-242.
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/H值/χ2值 | P值 |
|---|---|---|---|---|---|
| 年龄(岁) | 27.95±8.28 | 38.13±12.71* | 42.4±13.84*# | 14.738 | <0.01 |
| 性别[例(%)] | |||||
| 男 女 | 8(42.2) 11(57.8) | 124(46.4) 143(53.6) | 149(60.3)# 98(39.7)# | 10.810 | <0.01 |
| 收缩压(mmHg) | 119(110, 130) | 130(120, 142)* | 138(130, 150)*# | 45.073 | <0.01 |
| 舒张压(mmHg) | 71(68, 78) | 80(73, 90)* | 83(77, 92)*# | 22.211 | <0.01 |
| 激素或免疫抑制剂治疗[例(%)] | 7(36.8) | 76(28.5) | 73(29.6) | 0.965 | 0.617 |
| ACEI/ARB治疗[例(%)] | 2(10.5) | 110(41.2)* | 138(55.8)*# | 20.098 | <0.01 |
表1 3组一般资料比较
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/H值/χ2值 | P值 |
|---|---|---|---|---|---|
| 年龄(岁) | 27.95±8.28 | 38.13±12.71* | 42.4±13.84*# | 14.738 | <0.01 |
| 性别[例(%)] | |||||
| 男 女 | 8(42.2) 11(57.8) | 124(46.4) 143(53.6) | 149(60.3)# 98(39.7)# | 10.810 | <0.01 |
| 收缩压(mmHg) | 119(110, 130) | 130(120, 142)* | 138(130, 150)*# | 45.073 | <0.01 |
| 舒张压(mmHg) | 71(68, 78) | 80(73, 90)* | 83(77, 92)*# | 22.211 | <0.01 |
| 激素或免疫抑制剂治疗[例(%)] | 7(36.8) | 76(28.5) | 73(29.6) | 0.965 | 0.617 |
| ACEI/ARB治疗[例(%)] | 2(10.5) | 110(41.2)* | 138(55.8)*# | 20.098 | <0.01 |
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | H值/F值 | P值 |
|---|---|---|---|---|---|
| eGFR[ml/(min·1.73 m2)] | 100.3±24.24 | 85.69±30.76* | 80.62±27.72*# | 5.063 | <0.01 |
| 血红蛋白(g/L) | 126.4±20.39 | 128.8±19.74 | 136.7±18.79*# | 11.725 | <0.01 |
| 24小时尿蛋白排泄量(g/d) | 1.38(0.25, 1.98) | 1.13(0.58, 2.26) | 2.01(0.98, 3.55)*# | 35.348 | <0.01 |
| CRP(mg/L) | 1.99(1.15, 3.7) | 1.33(0.79, 2.20) | 1.88(1.05, 3.27)# | 15.372 | <0.01 |
| 中性粒细胞计数(×109/L) | 4.66(3.94, 6.29) | 3.61(2.90, 4.71)* | 3.96(3.14, 4.93) | 12.833 | <0.01 |
| TC(mmol/L) | 4.45(3.36, 5.04) | 4.81(4.17, 5.79) | 4.96(4.21, 6.21) | 5.468 | 0.065 |
| LDL-C(mmol/L) | 2.08(1.45, 2.91) | 2.95(2.41, 3.79)* | 3.14(2.44, 3.98)* | 12.098 | <0.01 |
| BUN(mmol/L) | 4.92(3.93, 6.0) | 5.88(4.60, 7.79) | 5.94(4.60, 7.52) | 4.417 | 0.110 |
| 血UA(μmol/L) | 314.7±102.6 | 354.1±98.88* | 385.40±94.62*# | 9.528 | <0.01 |
| TG(mmol/L) | 0.88(0.60, 1.37) | 1.19(0.88, 1.76) | 1.63(1.16, 2.43)*# | 46.493 | <0.01 |
| CysC(mg/L) | 0.94(0.81, 1.57) | 1.01(0.84, 1.34) | 1.09(0.88, 147) | 3.310 | 0.191 |
| HDL-C(mmol/L) | 1.45(1.22, 1.67) | 1.36(1.16, 1.64) | 1.18(1.02, 1.41)*# | 32.023 | <0.01 |
| FPG(mmol/L) | 4.3(3.99, 4.62) | 4.55(4.25, 4.85) | 4.77(4.34, 5.23)*# | 25.039 | <0.01 |
| 尿红细胞计数(个/μL) | 51(19.1, 109.3) | 65.34(22.8, 132.5) | 56.60(21.12, 117.1) | 1.842 | 0.398 |
| 尿白细胞计数(个/μL) | 5.94(3.5, 16.7) | 7.04(3.96, 13.8) | 6.70(3.30, 14.30) | 0.603 | 0.740 |
| C1q(mg/L) | 167(133.2, 202.3) | 179(155.8, 205.3) | 183(158.9, 205.4) | 3.257 | 0.196 |
| C3(g/L) | 0.88(0.73, 1.03) | 1.01(0.87, 1.14) | 1.12(1.01, 1.28)*# | 54.860 | <0.01 |
| C4(g/L) | 0.22(0.16, 0.26) | 0.23(0.19, 0.28) | 0.27(0.22, 0.32)*# | 29.190 | <0.01 |
| IgG(g/L) | 10.90±3.33 | 10.13±3.49 | 9.99±3.53 | 0.561 | 0.571 |
| IgE(IU/ml) | 59.49(17.16, 155.80) | 66.39(22.67, 149.70) | 50.34(21.93, 141.80) | 0.639 | 0.726 |
| IgA(g/L) | 3.14(2.37, 3.66) | 2.92(2.36, 3.68) | 3.04(2.32, 4.01) | 1.070 | 0.586 |
| IgM(g/L) | 1.04(0.86, 1.58) | 1.00(0.72, 1.41) | 0.89(0.62, 1.25)# | 8.643 | 0.013 |
表2 3组实验室资料比较
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | H值/F值 | P值 |
|---|---|---|---|---|---|
| eGFR[ml/(min·1.73 m2)] | 100.3±24.24 | 85.69±30.76* | 80.62±27.72*# | 5.063 | <0.01 |
| 血红蛋白(g/L) | 126.4±20.39 | 128.8±19.74 | 136.7±18.79*# | 11.725 | <0.01 |
| 24小时尿蛋白排泄量(g/d) | 1.38(0.25, 1.98) | 1.13(0.58, 2.26) | 2.01(0.98, 3.55)*# | 35.348 | <0.01 |
| CRP(mg/L) | 1.99(1.15, 3.7) | 1.33(0.79, 2.20) | 1.88(1.05, 3.27)# | 15.372 | <0.01 |
| 中性粒细胞计数(×109/L) | 4.66(3.94, 6.29) | 3.61(2.90, 4.71)* | 3.96(3.14, 4.93) | 12.833 | <0.01 |
| TC(mmol/L) | 4.45(3.36, 5.04) | 4.81(4.17, 5.79) | 4.96(4.21, 6.21) | 5.468 | 0.065 |
| LDL-C(mmol/L) | 2.08(1.45, 2.91) | 2.95(2.41, 3.79)* | 3.14(2.44, 3.98)* | 12.098 | <0.01 |
| BUN(mmol/L) | 4.92(3.93, 6.0) | 5.88(4.60, 7.79) | 5.94(4.60, 7.52) | 4.417 | 0.110 |
| 血UA(μmol/L) | 314.7±102.6 | 354.1±98.88* | 385.40±94.62*# | 9.528 | <0.01 |
| TG(mmol/L) | 0.88(0.60, 1.37) | 1.19(0.88, 1.76) | 1.63(1.16, 2.43)*# | 46.493 | <0.01 |
| CysC(mg/L) | 0.94(0.81, 1.57) | 1.01(0.84, 1.34) | 1.09(0.88, 147) | 3.310 | 0.191 |
| HDL-C(mmol/L) | 1.45(1.22, 1.67) | 1.36(1.16, 1.64) | 1.18(1.02, 1.41)*# | 32.023 | <0.01 |
| FPG(mmol/L) | 4.3(3.99, 4.62) | 4.55(4.25, 4.85) | 4.77(4.34, 5.23)*# | 25.039 | <0.01 |
| 尿红细胞计数(个/μL) | 51(19.1, 109.3) | 65.34(22.8, 132.5) | 56.60(21.12, 117.1) | 1.842 | 0.398 |
| 尿白细胞计数(个/μL) | 5.94(3.5, 16.7) | 7.04(3.96, 13.8) | 6.70(3.30, 14.30) | 0.603 | 0.740 |
| C1q(mg/L) | 167(133.2, 202.3) | 179(155.8, 205.3) | 183(158.9, 205.4) | 3.257 | 0.196 |
| C3(g/L) | 0.88(0.73, 1.03) | 1.01(0.87, 1.14) | 1.12(1.01, 1.28)*# | 54.860 | <0.01 |
| C4(g/L) | 0.22(0.16, 0.26) | 0.23(0.19, 0.28) | 0.27(0.22, 0.32)*# | 29.190 | <0.01 |
| IgG(g/L) | 10.90±3.33 | 10.13±3.49 | 9.99±3.53 | 0.561 | 0.571 |
| IgE(IU/ml) | 59.49(17.16, 155.80) | 66.39(22.67, 149.70) | 50.34(21.93, 141.80) | 0.639 | 0.726 |
| IgA(g/L) | 3.14(2.37, 3.66) | 2.92(2.36, 3.68) | 3.04(2.32, 4.01) | 1.070 | 0.586 |
| IgM(g/L) | 1.04(0.86, 1.58) | 1.00(0.72, 1.41) | 0.89(0.62, 1.25)# | 8.643 | 0.013 |
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/χ2值 | P值 |
|---|---|---|---|---|---|
| 男性 | |||||
| 例数 | 8 | 124 | 149 | ||
| 血红蛋白(g/L) | 126.1±19.25 | 138.9±19.05 | 142.6±16.64* | 4.269 | 0.015 |
| eGFR[ml/(min·1.73 m2)] | 99.56±34.77 | 83.23±32.39 | 79.36±26.61 | 1.947 | 0.145 |
| 血UA(μmol/L) | 382.9±120.7 | 397.6±96.8 | 409.6±95.2 | 0.554 | 0.575 |
| 女性 | |||||
| 例数 | 11 | 143 | 98 | ||
| 血红蛋白(g/L) | 126.5±22.11 | 120.0±15.77 | 127.0±15.55# | 2.711 | <0.01 |
| eGFR[ml/(min·1.73 m2)] | 100.8±14.51 | 87.83±29.23 | 81.96±29.21* | 5.767 | <0.01 |
| 血UA(μmol/L) | 265.2±48.33 | 316.4±84.41 | 350.6±85.42*# | 8.026 | <0.01 |
表3 按性别分层后3组UA、血红蛋白、eGFR比较
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/χ2值 | P值 |
|---|---|---|---|---|---|
| 男性 | |||||
| 例数 | 8 | 124 | 149 | ||
| 血红蛋白(g/L) | 126.1±19.25 | 138.9±19.05 | 142.6±16.64* | 4.269 | 0.015 |
| eGFR[ml/(min·1.73 m2)] | 99.56±34.77 | 83.23±32.39 | 79.36±26.61 | 1.947 | 0.145 |
| 血UA(μmol/L) | 382.9±120.7 | 397.6±96.8 | 409.6±95.2 | 0.554 | 0.575 |
| 女性 | |||||
| 例数 | 11 | 143 | 98 | ||
| 血红蛋白(g/L) | 126.5±22.11 | 120.0±15.77 | 127.0±15.55# | 2.711 | <0.01 |
| eGFR[ml/(min·1.73 m2)] | 100.8±14.51 | 87.83±29.23 | 81.96±29.21* | 5.767 | <0.01 |
| 血UA(μmol/L) | 265.2±48.33 | 316.4±84.41 | 350.6±85.42*# | 8.026 | <0.01 |
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/χ2值 | P值 |
|---|---|---|---|---|---|
| 免疫球蛋白沉积强度 | |||||
| IgG | 0.26±0.70 | 0.26±0.67 | 0.33±0.73 | 0.964 | 0.358 |
| IgA | 3.33±0.61 | 3.08±0.79 | 3.05±0.77 | 0.714 | 0.408 |
| IgM | 0.53±0.83 | 0.82±1.02 | 0.79±1.04 | 0.547 | 0.569 |
| 补体沉积强度 | |||||
| C3 | 2.13±0.99 | 2.04±1.11 | 1.78±1.18# | 3.848 | 0.035 |
| C1q | 0.14±0.54 | 0.09±0.37 | 0.08±0.36 | 0.422 | 0.615 |
| 炎细胞浸润程度 | 1.88±1.20 | 2.48±1.03* | 2.58±0.91* | 4.068 | 0.018 |
| 血管损伤程度 | 0.26±0.65 | 0.79±0.89* | 0.92±0.95* | 4.947 | 0.007 |
| 牛津病理分型[例(%)] | |||||
| M1 | 14(73.7) | 228(85.4) | 210(85.0) | 1.638 | 0.441 |
| E1 | 3(15.8) | 48(18.0) | 56(22.7) | 3.646 | 0.110 |
| S1 | 7(36.8) | 137(51.3) | 128(51.8) | 1.616 | 0.447 |
| T0 | 16(84.2) | 239(89.5) | 203(82.2) | 5.789 | 0.055 |
| T1+T2 | 3(15.8) | 28(10.5) | 44(17.8) | ||
| C0 | 14(73.7) | 225(84.3) | 215(87.0) | 2.560 | 0.278 |
| C1+C2 | 5(26.3) | 42(15.7) | 32(13.0) |
表4 3组肾脏病理改变的比较
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/χ2值 | P值 |
|---|---|---|---|---|---|
| 免疫球蛋白沉积强度 | |||||
| IgG | 0.26±0.70 | 0.26±0.67 | 0.33±0.73 | 0.964 | 0.358 |
| IgA | 3.33±0.61 | 3.08±0.79 | 3.05±0.77 | 0.714 | 0.408 |
| IgM | 0.53±0.83 | 0.82±1.02 | 0.79±1.04 | 0.547 | 0.569 |
| 补体沉积强度 | |||||
| C3 | 2.13±0.99 | 2.04±1.11 | 1.78±1.18# | 3.848 | 0.035 |
| C1q | 0.14±0.54 | 0.09±0.37 | 0.08±0.36 | 0.422 | 0.615 |
| 炎细胞浸润程度 | 1.88±1.20 | 2.48±1.03* | 2.58±0.91* | 4.068 | 0.018 |
| 血管损伤程度 | 0.26±0.65 | 0.79±0.89* | 0.92±0.95* | 4.947 | 0.007 |
| 牛津病理分型[例(%)] | |||||
| M1 | 14(73.7) | 228(85.4) | 210(85.0) | 1.638 | 0.441 |
| E1 | 3(15.8) | 48(18.0) | 56(22.7) | 3.646 | 0.110 |
| S1 | 7(36.8) | 137(51.3) | 128(51.8) | 1.616 | 0.447 |
| T0 | 16(84.2) | 239(89.5) | 203(82.2) | 5.789 | 0.055 |
| T1+T2 | 3(15.8) | 28(10.5) | 44(17.8) | ||
| C0 | 14(73.7) | 225(84.3) | 215(87.0) | 2.560 | 0.278 |
| C1+C2 | 5(26.3) | 42(15.7) | 32(13.0) |
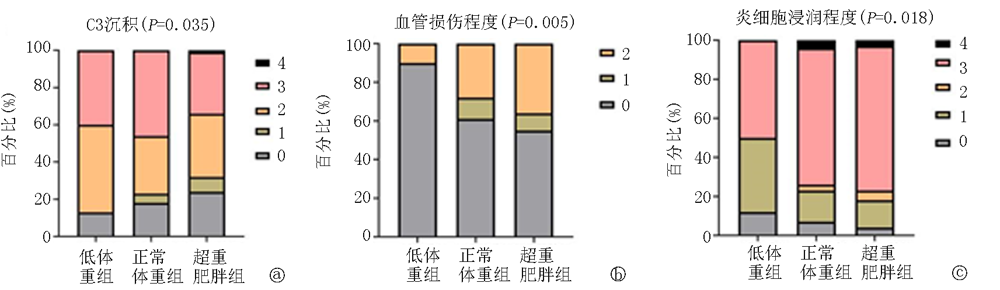
图1 3组C3沉积、血管损伤程度、炎细胞浸润程度比较 a.C3沉积; b.炎细胞浸润程度; c.血管损伤程度

图2 3组Kaplan-Meier生存曲线
| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | HR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 年龄 | -0.018 | 0.019 | 0.874 | 0.350 | 0.98 | 0.94 | 1.02 |
| 性别 | 0.561 | 0.499 | 1.262 | 0.261 | 1.75 | 0.66 | 4.66 |
| BMI | 0.136 | 0.077 | 3.115 | 0.049 | 1.17 | 1.00 | 1.36 |
| eGFR | -0.040 | 0.013 | 10.276 | 0.001 | 0.96 | 0.93 | 0.98 |
| 24小时尿蛋白排泄量 | 0.205 | 0.082 | 6.219 | 0.013 | 1.23 | 1.04 | 1.44 |
| 血红蛋白 | -0.042 | 0.011 | 15.790 | 0.000 | 0.96 | 0.94 | 0.98 |
| 血UA | 0.005 | 0.003 | 3.729 | 0.052 | 1.01 | 1.00 | 1.10 |
| TG | 0.275 | 0.135 | 4.125 | 0.042 | 1.32 | 1.01 | 1.72 |
| C3 | 0.510 | 0.946 | 0.291 | 0.573 | 1.79 | 0.23 | 13.86 |
| 肾小管萎缩/间质纤维化比例≥25% | 0.777 | 0.327 | 5.641 | 0.018 | 3.44 | 1.23 | 9.59 |
| 炎细胞浸润程度 | 0.375 | 0.311 | 1.454 | 0.228 | 1.45 | 0.79 | 2.67 |
| 激素和(或)免疫抑制剂治疗 | -0.164 | 0.485 | 0.115 | 0.610 | 0.79 | 0.32 | 1.97 |
| ACEI/ARB治疗 | 0.308 | 0.468 | 0.434 | 0.510 | 1.36 | 0.54 | 3.41 |
表5 影响IgAN合并超重肥胖肾脏预后的Cox单因素分析
| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | HR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 年龄 | -0.018 | 0.019 | 0.874 | 0.350 | 0.98 | 0.94 | 1.02 |
| 性别 | 0.561 | 0.499 | 1.262 | 0.261 | 1.75 | 0.66 | 4.66 |
| BMI | 0.136 | 0.077 | 3.115 | 0.049 | 1.17 | 1.00 | 1.36 |
| eGFR | -0.040 | 0.013 | 10.276 | 0.001 | 0.96 | 0.93 | 0.98 |
| 24小时尿蛋白排泄量 | 0.205 | 0.082 | 6.219 | 0.013 | 1.23 | 1.04 | 1.44 |
| 血红蛋白 | -0.042 | 0.011 | 15.790 | 0.000 | 0.96 | 0.94 | 0.98 |
| 血UA | 0.005 | 0.003 | 3.729 | 0.052 | 1.01 | 1.00 | 1.10 |
| TG | 0.275 | 0.135 | 4.125 | 0.042 | 1.32 | 1.01 | 1.72 |
| C3 | 0.510 | 0.946 | 0.291 | 0.573 | 1.79 | 0.23 | 13.86 |
| 肾小管萎缩/间质纤维化比例≥25% | 0.777 | 0.327 | 5.641 | 0.018 | 3.44 | 1.23 | 9.59 |
| 炎细胞浸润程度 | 0.375 | 0.311 | 1.454 | 0.228 | 1.45 | 0.79 | 2.67 |
| 激素和(或)免疫抑制剂治疗 | -0.164 | 0.485 | 0.115 | 0.610 | 0.79 | 0.32 | 1.97 |
| ACEI/ARB治疗 | 0.308 | 0.468 | 0.434 | 0.510 | 1.36 | 0.54 | 3.41 |
| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | HR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 24小时尿蛋白排泄量 | 0.203 | 0.097 | 4.404 | 0.035 | 1.23 | 1.01 | 1.48 |
| 血红蛋白 | -0.077 | 0.015 | 25.641 | 0.0001 | 0.93 | 0.89 | 0.95 |
| TG | 0.432 | 0.180 | 5.765 | 0.015 | 1.55 | 1.09 | 2.21 |
表6 影响IgAN合并超重肥胖肾脏预后的Cox多因素分析
| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | HR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 24小时尿蛋白排泄量 | 0.203 | 0.097 | 4.404 | 0.035 | 1.23 | 1.01 | 1.48 |
| 血红蛋白 | -0.077 | 0.015 | 25.641 | 0.0001 | 0.93 | 0.89 | 0.95 |
| TG | 0.432 | 0.180 | 5.765 | 0.015 | 1.55 | 1.09 | 2.21 |
| [1] |
Rajasekaran A, Julian BA, Rizk DV. IgA nephropathy: An interesting autoimmune kidney disease[J]. Am J Med Sci, 2021, 361(2):176-194.
doi: 10.1016/j.amjms.2020.10.003 pmid: 33309134 |
| [2] |
Roberts IS. Pathology of IgA nephropathy[J]. Nat Rev Nephrol, 2014, 10(8):445-454.
doi: 10.1038/nrneph.2014.92 pmid: 24861083 |
| [3] |
Mohd R, Mohammad Kazmin NE, Abdul Cader R, et al. Long term outcome of immunoglobulin A (IgA) nephropathy: A single center experience[J]. PLoS One, 2021, 16(4):e0249592.
doi: 10.1371/journal.pone.0249592 URL |
| [4] |
Matsuzaki K, Suzuki H, Kawamura T, et al. Utility of remission criteria for the renal prognosis of IgA nephropathy[J]. Clin Exp Nephrol, 2021, 25(9):988-995.
doi: 10.1007/s10157-021-02069-w pmid: 33974158 |
| [5] |
Sagi B, Késõi I, Vas T, et al. The prognostic role of heart rate recovery after exercise and metabolic syndrome in IgA nephropathy[J]. BMC Nephrol, 2021, 22(1):390.
doi: 10.1186/s12882-021-02596-4 URL |
| [6] |
Lu P, Li X, Zhu N, et al. Serum uric acid level is correlated with the clinical, pathological progression and prognosis of IgA nephropathy: An observational retrospective pilot-study[J]. PeerJ, 2020, 8:e10130.
doi: 10.7717/peerj.10130 URL |
| [7] |
Zheng Y, Wang Y, Liu SW, et al. Potential blood pressure goals in IgA nephropathy: Prevalence, awareness, and treatment rates in chronic kidney disease among patients with hypertension in China (PATRIOTIC) study[J]. Kidney Blood Press Res, 2018, 43(6):1786-1795.
doi: 10.1159/000495636 URL |
| [8] |
Zheng W, Mclerran DF, Rolland B, et al. Association between body-mass index and risk of death in more than 1 million Asians[J]. New Engl J Med, 2011, 364(8):719-729.
doi: 10.1056/NEJMoa1010679 URL |
| [9] |
Kataoka H, Ohara M, Shibui K, et al. Overweight and obesity accelerate the progression of IgA nephropathy: Prognostic utility of a combination of BMI and histopathological parameters[J]. Clin Exp Nephrol, 2012, 16(5):706-712.
doi: 10.1007/s10157-012-0613-7 URL |
| [10] |
Wu C, Wang AY, Li G, et al. Association of high body mass index with development of interstitial fibrosis in patients with IgA nephropathy[J]. BMC Nephrol, 2018, 19(1):381.
doi: 10.1186/s12882-018-1164-2 URL |
| [11] |
Ouyang Y, Xie J, Yang M, et al. Underweight is an independent risk factor for renal function deterioration in patients with IgA nephropathy[J]. PLoS One, 2016, 11(9):e0162044.
doi: 10.1371/journal.pone.0162044 URL |
| [12] |
Kikuchi H, Kanda E, Mandai S, et al. Combination of low body mass index and serum albumin level is associated with chronic kidney disease progression: The chronic kidney disease-research of outcomes in treatment and epidemiology (CKD-ROUTE) study[J]. Clin Exp Nephrol, 2017, 21(1):55-62.
doi: 10.1007/s10157-016-1251-2 URL |
| [13] |
Yun HR, Kim H, Park JT, et al. Obesity, metabolic abnormality, and progression of CKD[J]. Am J Kidney Dis, 2018, 72(3):400-410.
doi: 10.1053/j.ajkd.2018.02.362 URL |
| [14] | 裴改琴, 秦嫒雅, 王思清, 等. 血清IgA/C3和病理C3沉积对IgA肾病患者临床预后的影响[J]. 中华医学杂志, 2020, 100(30):2372-2377. |
| [15] |
Jarrick S, Lundberg S, Welander A, et al. Mortality in IgA nephropathy: A nationwide population-based cohort study[J]. J Am Soc Nephrol, 2019, 30(5):866-876.
doi: 10.1681/ASN.2018101017 pmid: 30971457 |
| [16] |
Wang Y, Zhao L, Gao L, et al. Health policy and public health implications of obesity in China[J]. Lancet Diabetes Endocrinol, 2021, 9(7):446-461.
doi: 10.1016/S2213-8587(21)00118-2 URL |
| [17] |
Pan XF, Wang LM, Pan A. Epidemiology and determinants of obesity in China[J]. Lancet Diabetes Endocrinol, 2021, 9(6):373-392.
doi: 10.1016/S2213-8587(21)00045-0 URL |
| [18] |
Lai YJ, Hu HY, Lee YL, et al. Association between obesity and risk of chronic kidney disease: A nationwide cohort study in Taiwan[J]. Nutr Metab Cardiovasc Dis, 2017, 27(11):1008-1014.
doi: S0939-4753(17)30200-4 pmid: 28986076 |
| [19] |
Wang Y, Chen X, Song Y, et al. Association between obesity and kidney disease: A systematic review and meta-analysis[J]. Kidney Int, 2008, 73(1):19-33.
pmid: 17928825 |
| [20] |
Zoccali C. The obesity epidemics in ESRD: From wasting to waist?[J]. Nephrol Dial Transplant, 2009, 24(2):376-380.
doi: 10.1093/ndt/gfn589 URL |
| [21] |
Berthoux F, Mohey H, Laurent B, et al. Predicting the risk for dialysis or death in IgA nephropathy[J]. J Am Soc Nephrol, 2011, 22(4):752-761.
doi: 10.1681/ASN.2010040355 URL |
| [22] |
Choi WJ, Hong YA, Min JW, et al. The serum uric acid level is related to the more severe renal histopathology of female IgA nephropathy patients[J]. J Clin Med, 2021, 10(9) : 1885.
doi: 10.3390/jcm10091885 URL |
| [23] |
Yonekura Y, Goto S, Sugiyama H, et al. The influences of larger physical constitutions including obesity on the amount of urine protein excretion in primary glomerulonephritis: Research of the Japan renal biopsy registry[J]. Clin Exp Nephrol, 2015, 19(3):359-370.
doi: 10.1007/s10157-014-0993-y pmid: 24916004 |
| [24] |
Fox CS, Larson MG, Leip EP, et al. Predictors of new-onset kidney disease in a community-based population[J]. JAMA, 2004, 291(7):844-850.
doi: 10.1001/jama.291.7.844 URL |
| [25] |
Kalaitzidis RG, Siamopoulos KC. The role of obesity in kidney disease: Recent findings and potential mechanisms[J]. Int Urol Nephrol, 2011, 43(3):771-784.
doi: 10.1007/s11255-011-9974-1 pmid: 21544651 |
| [26] |
Tanaka M, Yamada S, Iwasaki Y, et al. Impact of obesity on IgA nephropathy: Comparative ultrastructural study between obese and non-obese patients[J]. Nephron Clin Pract, 2009, 112(2):c71-c78.
doi: 10.1159/000213084 URL |
| [27] |
Gabrielsson BG, Johansson JM, Lonn M, et al. High expression of complement components in omental adipose tissue in obese men[J]. Obes Res, 2003, 11(6):699-708.
pmid: 12805391 |
| [28] |
Karkhaneh M, Qorbani M, Mohajeri-Tehrani MR, et al. Association of serum complement C3 with metabolic syndrome components in normal weight obese women[J]. J Diabetes Metab Disord, 2017, 16:49.
doi: 10.1186/s40200-017-0330-6 URL |
| [29] |
Ohsawa I, Inoshita H, Ishii M, et al. Metabolic impact on serum levels of complement component 3 in Japanese patients[J]. J Clin Lab Anal, 2010, 24(2):113-118.
doi: 10.1002/jcla.20372 pmid: 20333766 |
| [30] |
Wlazlo N, van Greevenbroek MM, Ferreira I, et al. Low-grade inflammation and insulin resistance independently explain substantial parts of the association between body fat and serum C3: The CODAM study[J]. Metabolism, 2012, 61(12):1787-1796.
doi: 10.1016/j.metabol.2012.05.015 URL |
| [31] |
Al Haj Ahmad RM, Al-Domi HA. Complement 3 serum levels as a pro-inflammatory biomarker for insulin resistance in obesity[J]. Diabetes Metab Syndr, 2017, 11:S229-S232.
doi: 10.1016/j.dsx.2016.12.036 URL |
| [32] |
Engstrom G, Hedblad B, Janzon L, et al. Weight gain in relation to plasma levels of complement factor 3: Results from a population-based cohort study[J]. Diabetologia, 2005, 48(12):2525-2531.
doi: 10.1007/s00125-005-0021-6 URL |
| [33] |
Harmon DB, Srikakulapu P, Kaplan JL, et al. Protective role for B-1b B cells and IgM in obesity-associated inflammation, glucose intolerance, and insulin resistance[J]. Arterioscler Thromb Vasc Biol, 2016, 36(4):682-691.
doi: 10.1161/ATVBAHA.116.307166 URL |
| [34] |
Stefan G, Ismail G, Stancu S, et al. Validation study of Oxford classification of IgA nephropathy: The significance of extracapillary hypercellularity and mesangial IgG immunostaining[J]. Pathol Int, 2016, 66(8):453-459.
doi: 10.1111/pin.2016.66.issue-8 URL |
| [35] |
Hong YA, Min JW, Ha MA, et al. The impact of obesity on the severity of clinicopathologic parameters in patients with IgA nephropathy[J]. J Clin Med, 2020, 9(9) : 2824.
doi: 10.3390/jcm9092824 URL |
| [36] |
Nam KH, Joo YS, Lee C, et al. Predictive value of mesangial C3 and C4d deposition in IgA nephropathy[J]. Clin Immunol, 2020, 211:108331.
doi: 10.1016/j.clim.2019.108331 URL |
| [37] |
Park S, Kim HW, Park JT, et al. Relationship between complement deposition and the Oxford classification score and their combined effects on renal outcome in immunoglobulin A nephropathy[J]. Nephrol Dial Transplant, 2020, 35(12):2103-2137.
doi: 10.1093/ndt/gfz179 URL |
| [38] |
Lee H, Kim DK, Oh KH, et al. Mortality of IgA nephropathy patients: A single center experience over 30 years[J]. PLoS One, 2012, 7(12):e51225.
doi: 10.1371/journal.pone.0051225 URL |
| [39] |
Le W, Liang S, Hu Y, et al. Long-term renal survival and related risk factors in patients with IgA nephropathy: Results from a cohort of 1155 cases in a Chinese adult population[J]. Nephrol Dial Transpl, 2012, 27(4):1479-1485.
doi: 10.1093/ndt/gfr527 URL |
| [40] |
Praga M, Morales E. Obesity, proteinuria and progression of renal failure[J]. Curr Opin Nephrol Hypertens, 2006, 15(5):481-486.
doi: 10.1097/01.mnh.0000242172.06459.7c URL |
| [41] |
Al-Hashem FH. Is it necessary to consider obesity when constructing norms for hemoglobin or when screening for anemia using hemoglobin levels?[J]. Saudi Med J, 2007, 28(1):41-45.
pmid: 17206287 |
| [42] |
Theodore B. Health implications of overweight and obesity in the United States[J]. Ann Intern Med, 1985, 103:983-988.
doi: 10.7326/0003-4819-103-6-983 URL |
| [43] |
Oh TR, Song SH, Choi HS, et al. The association between serum hemoglobin and renal prognosis of IgA nephropathy[J]. J Clin Med, 2021, 10(2):363.
doi: 10.3390/jcm10020363 URL |
| [44] |
Zhu B, Liu WH, Yu DR, et al. The association of low hemoglobin levels with IgA nephropathy progression: A two-center cohort study of 1, 828 cases[J]. Am J Nephrol, 2020, 51(8):624-634.
doi: 10.1159/000508770 URL |
| [45] |
van Iterson EH, Kim CH, Uithoven K, et al. Obesity and hemoglobin content impact peak oxygen uptake in human heart failure[J]. Eur J Prev Cardiol, 2018, 25(18):1937-1946.
doi: 10.1177/2047487318802695 pmid: 30247068 |
| [1] | 赵旭辉, 黄小敏, 达德转, 许焱, 崔晓东, 李红玲. 基于生物信息学筛选影响胃癌患者预后的糖酵解相关基因[J]. 临床荟萃, 2024, 39(1): 20-29. |
| [2] | 刘丽丽, 袁宇婷, 赖耿良, 田川, 蓝翔, 叶中绿. 儿童急性淋巴细胞白血病第15天微小残留与预后的关系[J]. 临床荟萃, 2024, 39(1): 47-52. |
| [3] | 崔兰丹, 杨春燕. 脓毒症患者甲状腺激素的变化特点及研究进展[J]. 临床荟萃, 2024, 39(1): 70-74. |
| [4] | 王涛, 高玉伟, 王兴华, 胡秀红, 崔红蕊, 徐保振, 杨洪娟. 抗磷脂酶A2受体抗体与特发性膜性肾病的相关性[J]. 临床荟萃, 2023, 38(7): 606-612. |
| [5] | 高秦宇, 包蓓艳, 金燕, 赵宇. IgA肾病合并抑郁状态患者的临床特征和预后影响因素分析[J]. 临床荟萃, 2023, 38(6): 510-515. |
| [6] | 孙星星, 林海. 儿童重症肺炎的免疫功能变化及预后危险因素[J]. 临床荟萃, 2023, 38(6): 521-525. |
| [7] | 贺翔渝, 潘燕, 张小林. 血清脂蛋白相关磷脂酶A2水平与急性缺血性脑卒中病情及预后的关系[J]. 临床荟萃, 2023, 38(4): 315-318. |
| [8] | 杨金强, 张仁敏. 降钙素原与血小板比值评估发热伴血小板减少综合征预后的价值[J]. 临床荟萃, 2023, 38(4): 346-351. |
| [9] | 罗杰, 吴强, 李忠, 郑硕. 罕见肾上腺神经纤维瘤1例并文献复习[J]. 临床荟萃, 2023, 38(4): 359-363. |
| [10] | 张娜, 孙越, 董晗, 赵鹏, 杨昕, 祁源, 王玲玲. SPARC表达水平与非小细胞肺癌患者预后关系的meta分析[J]. 临床荟萃, 2023, 38(11): 972-978. |
| [11] | 王会新, 赵芳晴, 张馨妍, 侯晓雯. 中国人尿酸水平与急性缺血性脑卒中患者预后关系的meta分析[J]. 临床荟萃, 2022, 37(9): 785-790. |
| [12] | 邢婷婷, 高俊茶. Presepsin在急性胰腺炎中的研究进展[J]. 临床荟萃, 2022, 37(8): 764-768. |
| [13] | 轩晓倩, 赵君慧, 杨小茜. 炎性指标在非小细胞肺癌患者预后中的临床意义[J]. 临床荟萃, 2022, 37(7): 663-667. |
| [14] | 叶倩, 凌志, 刘申香, 路国涛, 殷旭东. 糖皮质激素对晚期肿瘤患者免疫疗效影响的Meta分析[J]. 临床荟萃, 2022, 37(7): 591-598. |
| [15] | 周彬, 曾词正, 黄宇戈, 钟娩玲, 吴家园. pSOFA评分联合C-反应蛋白、降钙素原在脓毒症患儿预后评估中的作用[J]. 临床荟萃, 2022, 37(7): 616-622. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||