Clinical Focus ›› 2021, Vol. 36 ›› Issue (3): 256-261.doi: 10.3969/j.issn.1004-583X.2021.03.014
Previous Articles Next Articles
Treatment and prognosis of malignant hypertension complicated with thrombotic microangiopathy for young IgAN patients
Di Dingxin1, Zhang Zheng2, Li Yetong3, Zou Guming2, Gao Hongmei2, Li Wenge1,2( )
)
- 1. Graduate School of Peking Union Medical College, China-Japan Friendship School of Clinical Medicine, Beijing 100029, China
2. Department of Nephropathy, China-Japan Friendship Hospital,Beijing 100029, China
3. Capital Medical University, Beijing 100045, China
-
Received:2020-12-24Online:2021-03-20Published:2021-03-29 -
Contact:Li Wenge E-mail:wenge_lee2002@126.com
CLC Number:
Cite this article
Di Dingxin, Zhang Zheng, Li Yetong, Zou Guming, Gao Hongmei, Li Wenge. Treatment and prognosis of malignant hypertension complicated with thrombotic microangiopathy for young IgAN patients[J]. Clinical Focus, 2021, 36(3): 256-261.
share this article
Add to citation manager EndNote|Ris|BibTeX
URL: https://huicui.hebmu.edu.cn/EN/10.3969/j.issn.1004-583X.2021.03.014
| 编号 | 年龄 (岁) | 性别 | 入院血压 (mmHg) | HGB (g/L) | PLT (×109/L) | SCr (μmol/L) | 24h-UPRO (g/d) | 尿红细胞 (个/HPF) | eGFR* | 进入 ESRD | 眼底(高血压性 视网膜病变) |
|---|---|---|---|---|---|---|---|---|---|---|---|
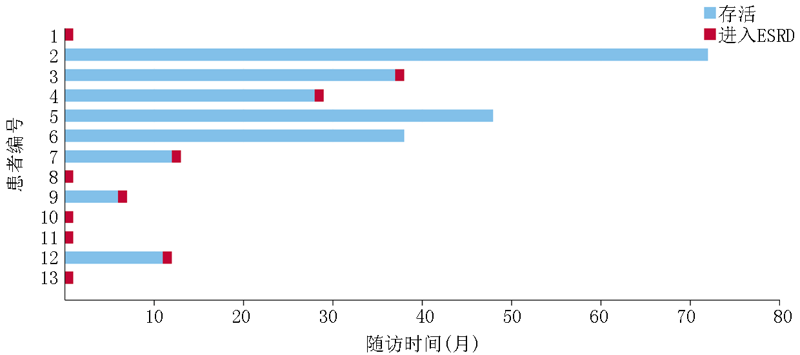
| 1 | 33 | 男 | 210/110 | 85 | 149 | 2170.0 | 1.73 | 30.0 | 2.35 | 是 | 双眼4级 |
| 2 | 27 | 男 | 240/140 | 150 | 220 | 129.0 | 0.21 | 0.2 | 60.22 | 否 | 右眼3级,左眼2级 |
| 3 | 32 | 男 | 190/120 | 136 | 213 | 268.0 | 3.13 | 1.9 | 27.39 | 否 | 双眼2级 |
| 4 | 24 | 男 | 206/100 | 121 | 212 | 269.2 | 1.80 | 23.8 | 23.82 | 否 | 右眼3级,左眼2级 |
| 5 | 34 | 男 | 190/140 | 155 | 208 | 149.5 | 0.50 | 6.1 | 53.14 | 否 | 双眼4级 |
| 6 | 26 | 男 | 180/140 | 156 | 282 | 178.3 | 4.40 | 17.7 | 41.82 | 否 | 右眼3级,左眼4级 |
| 7 | 28 | 男 | 200/130 | 120 | 148 | 541.6 | 7.58 | 8.5 | 11.37 | 是 | 右眼3级,左眼4级 |
| 8 | 25 | 男 | 195/150 | 68 | 136 | 1412.0 | 2.19 | 6.9 | 4.33 | 是 | 双眼3级 |
| 9 | 33 | 女 | 180/100 | 117 | 190 | 330.3 | 4.44 | 31.1 | 14.82 | 是 | 双眼3级 |
| 10 | 30 | 男 | 225/130 | 104 | 175 | 872.8 | 4.52 | 32.6 | 7.06 | 是 | 双眼3级 |
| 11 | 27 | 女 | 200/110 | 89 | 160 | 598.4 | 3.81 | 54.5 | 8.51 | 是 | 双眼3级 |
| 12 | 29 | 男 | 200/160 | 136 | 194 | 319.3 | 5.78 | 7.0 | 22.67 | 否 | 双眼4级 |
| 13 | 28 | 女 | 207/140 | 98 | 271 | 333.6 | 2.64 | 17.8 | 14.86 | 是 | 右眼2级,左眼3级 |
| 编号 | 年龄 (岁) | 性别 | 入院血压 (mmHg) | HGB (g/L) | PLT (×109/L) | SCr (μmol/L) | 24h-UPRO (g/d) | 尿红细胞 (个/HPF) | eGFR* | 进入 ESRD | 眼底(高血压性 视网膜病变) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 33 | 男 | 210/110 | 85 | 149 | 2170.0 | 1.73 | 30.0 | 2.35 | 是 | 双眼4级 |
| 2 | 27 | 男 | 240/140 | 150 | 220 | 129.0 | 0.21 | 0.2 | 60.22 | 否 | 右眼3级,左眼2级 |
| 3 | 32 | 男 | 190/120 | 136 | 213 | 268.0 | 3.13 | 1.9 | 27.39 | 否 | 双眼2级 |
| 4 | 24 | 男 | 206/100 | 121 | 212 | 269.2 | 1.80 | 23.8 | 23.82 | 否 | 右眼3级,左眼2级 |
| 5 | 34 | 男 | 190/140 | 155 | 208 | 149.5 | 0.50 | 6.1 | 53.14 | 否 | 双眼4级 |
| 6 | 26 | 男 | 180/140 | 156 | 282 | 178.3 | 4.40 | 17.7 | 41.82 | 否 | 右眼3级,左眼4级 |
| 7 | 28 | 男 | 200/130 | 120 | 148 | 541.6 | 7.58 | 8.5 | 11.37 | 是 | 右眼3级,左眼4级 |
| 8 | 25 | 男 | 195/150 | 68 | 136 | 1412.0 | 2.19 | 6.9 | 4.33 | 是 | 双眼3级 |
| 9 | 33 | 女 | 180/100 | 117 | 190 | 330.3 | 4.44 | 31.1 | 14.82 | 是 | 双眼3级 |
| 10 | 30 | 男 | 225/130 | 104 | 175 | 872.8 | 4.52 | 32.6 | 7.06 | 是 | 双眼3级 |
| 11 | 27 | 女 | 200/110 | 89 | 160 | 598.4 | 3.81 | 54.5 | 8.51 | 是 | 双眼3级 |
| 12 | 29 | 男 | 200/160 | 136 | 194 | 319.3 | 5.78 | 7.0 | 22.67 | 否 | 双眼4级 |
| 13 | 28 | 女 | 207/140 | 98 | 271 | 333.6 | 2.64 | 17.8 | 14.86 | 是 | 右眼2级,左眼3级 |
| 临床指标 | 值 |
|---|---|
| 年龄(岁) | 28.92±3.25 |
| 性别(男/女,例) | 10/3 |
| SBP(mmHg) | 201.77±16.82 |
| DBP(mmHg) | 128.46±19.08 |
| 尿红细胞(个/HPF) | 17.7(6.50, 30.55)* |
| 24h-UPRO(g/24 h) | 3.13(1.77, 4.48)* |
| SCr(μmol/L) | 330.3(223.2, 735.6)* |
| 尿酸(μmol/L) | 533.31±150.58 |
| HGB(g/L) | 118.08±28.173 |
| PLT(×109/L) | 196.77±44.88 |
| 血清IgA(mg/dL) | 276.5±91.4 |
| 补体C3(mg/dL) | 80.7±18.1 |
| 临床指标 | 值 |
|---|---|
| 年龄(岁) | 28.92±3.25 |
| 性别(男/女,例) | 10/3 |
| SBP(mmHg) | 201.77±16.82 |
| DBP(mmHg) | 128.46±19.08 |
| 尿红细胞(个/HPF) | 17.7(6.50, 30.55)* |
| 24h-UPRO(g/24 h) | 3.13(1.77, 4.48)* |
| SCr(μmol/L) | 330.3(223.2, 735.6)* |
| 尿酸(μmol/L) | 533.31±150.58 |
| HGB(g/L) | 118.08±28.173 |
| PLT(×109/L) | 196.77±44.88 |
| 血清IgA(mg/dL) | 276.5±91.4 |
| 补体C3(mg/dL) | 80.7±18.1 |
| 牛津分型病理指标 | 分型 | 例(%) |
|---|---|---|
| 系膜细胞增生(M) | M0 | 4(30.8) |
| M1 | 9(69.2) | |
| 肾小球节段硬化/球囊黏连(S) | S0 | 4(30.8) |
| S1 | 9(69.2) | |
| 毛细血管内增生(E) | E0 | 7(53.8) |
| E1 | 6(46.2) | |
| 肾小管萎缩/间质纤维化(T) | T0 | 1(7.7) |
| T1 | 3(23.1) | |
| T2 | 9(69.2) | |
| 新月体形成(C) | C0 | 2(15.4) |
| C1 | 10(76.9) | |
| C2 | 1(7.7) |
| 牛津分型病理指标 | 分型 | 例(%) |
|---|---|---|
| 系膜细胞增生(M) | M0 | 4(30.8) |
| M1 | 9(69.2) | |
| 肾小球节段硬化/球囊黏连(S) | S0 | 4(30.8) |
| S1 | 9(69.2) | |
| 毛细血管内增生(E) | E0 | 7(53.8) |
| E1 | 6(46.2) | |
| 肾小管萎缩/间质纤维化(T) | T0 | 1(7.7) |
| T1 | 3(23.1) | |
| T2 | 9(69.2) | |
| 新月体形成(C) | C0 | 2(15.4) |
| C1 | 10(76.9) | |
| C2 | 1(7.7) |
| [1] |
Markowitz G. Glomerular disease: Updated Oxford Classification of IgA nephropathy: a new MEST-C score[J]. Nat Rev Nephrol, 2017,13(7):385-386.
doi: 10.1038/nrneph.2017.67 pmid: 28529339 |
| [2] |
Chen T, Xia E, Chen T, et al. Identification and external validation of IgA nephropathy patients benefiting from immunosuppression therapy[J]. EBioMedicine, 2020,52:102657.
doi: 10.1016/j.ebiom.2020.102657 URL |
| [3] |
Jiang L, Zhang JJ, Lv JC, et al. Malignant hypertension in IgA nephropathy was not associated with background pathological phenotypes of glomerular lesions[J]. Nephrol Dial Transplant, 2008,23(12):3921-3927.
doi: 10.1093/ndt/gfn371 URL |
| [4] |
Timmermans S, Abdul-Hamid MA, Vanderlocht J, et al. Patients with hypertension-associated thrombotic microangiopathy may present with complement abnormalities[J]. Kidney Int, 2017,91(6):1420-1425.
doi: 10.1016/j.kint.2016.12.009 URL |
| [5] |
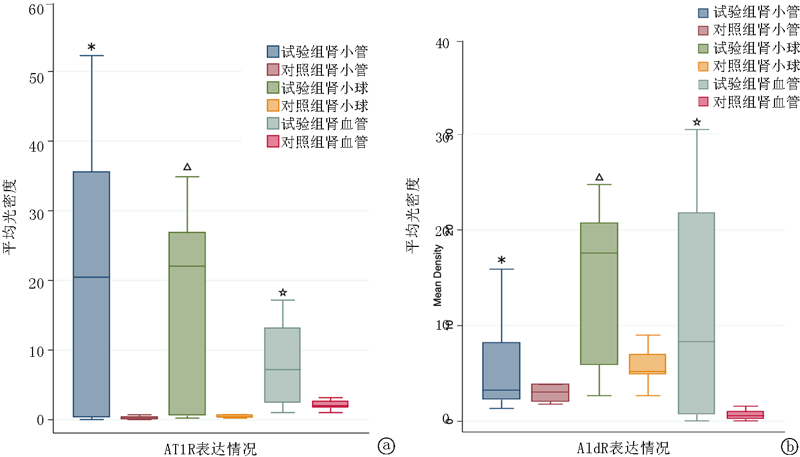
Zhang Z, Jiang SM, Ma YP, et al. Expression of the intrarenal angiotensin receptor and the role of renin-angiotensin system inhibitors in IgA nephropathy[J]. Mol Cell Biochem, 2019,453(1-2):103-110.
doi: 10.1007/s11010-018-3435-4 URL |
| [6] |
Trimarchi H, Barratt J, Cattran DC, et al. Oxford Classification of IgA nephropathy 2016: an update from the IgA Nephropathy Classification Working Group[J]. Kidney Int, 2017,91(5):1014-1021.
doi: 10.1016/j.kint.2017.02.003 URL |
| [7] | Yang Y, Zhang Z, Zhuo L, et al. The Spectrum of biopsy-proven glomerular disease in China: A systematic review[J]. Chin Med J (Engl), 2018,131(6):731-735. |
| [8] |
Barbour SJ, Coppo R, Zhang H, et al. Evaluating a new international risk-prediction tool in IgA nephropathy[J]. JAMA Intern Med, 2019,179(7):942-952.
doi: 10.1001/jamainternmed.2019.0600 pmid: 30980653 |
| [9] |
Unger T, Borghi C, Charchar F, et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines[J]. Hypertension, 2020,75(6):1334-1357.
doi: 10.1161/HYPERTENSIONAHA.120.15026 URL |
| [10] |
Mathew RO, Nayer A, Asif A. The endothelium as the common denominator in malignant hypertension and thrombotic microangiopathy[J]. J Am Soc Hypertens, 2016,10(4):352-359.
doi: 10.1016/j.jash.2015.12.007 pmid: 26778772 |
| [11] |
Cavero T, Arjona E, Soto K, et al. Severe and malignant hypertension are common in primary atypical hemolytic uremic syndrome[J]. Kidney Int, 2019,96(4):995-1004.
doi: 10.1016/j.kint.2019.05.014 URL |
| [12] |
Nagayama Y, Inoue Y, Inui K, et al. Comparison of renal outcome among Japanese patients with or without microangiopathic hemolysis in malignant phase hypertension: A single-center retrospective study[J]. Nephron, 2017,137(3):197-204.
doi: 10.1159/000479073 URL |
| [13] |
Timmermans S, Werion A, Damoiseaux J, et al. Diagnostic and risk factors for complement defects in hypertensive emergency and thrombotic microangiopathy[J]. Hypertension, 2020,75(2):422-430.
doi: 10.1161/HYPERTENSIONAHA.119.13714 pmid: 31865800 |
| [14] |
Abu Hamad R, Berman S, Hachmo Y, et al. Response of renal podocytes to excessive hydrostatic pressure: A pathophysiologic cascade in a malignant hypertension model[J]. Kidney Blood Press Res, 2017,42(6):1104-1118.
doi: 10.1159/000485774 URL |
| [15] |
Karnik SS, Unal H, Kemp JR, et al. International union of basic and clinical pharmacology. XCIX. Angiotensin receptors: Interpreters of pathophysiological angiotensinergic stimuli [corrected][J]. Pharmacol Rev, 2015,67(4):754-819.
doi: 10.1124/pr.114.010454 URL |
| [16] |
Itami H, Hara S, Samejima K, et al. Complement activation is associated with crescent formation in IgA nephropathy[J]. Virchows Arch, 2020,477(4):565-572.
doi: 10.1007/s00428-020-02800-0 URL |
| [17] |
Peng W, Tang Y, Tan L, et al. Crescents and global glomerulosclerosis in Chinese IgA nephropathy patients: A five-year follow-up[J]. Kidney Blood Press Res, 2019,44(1):103-112.
doi: 10.1159/000498874 URL |
| [18] |
Park S, Kim H W, Park J T, et al. Relationship between complement deposition and the Oxford classification score and their combined effects on renal outcome in immunoglobulin A nephropathy[J]. Nephrol Dial Transplant, 2020,35(12):2103-2137.
doi: 10.1093/ndt/gfz179 URL |
| [19] |
Alamartine E, Sauron C, Laurent B, et al. The use of the Oxford classification of IgA nephropathy to predict renal survival[J]. Clin J Am Soc Nephrol, 2011,6(10):2384-2388.
doi: 10.2215/CJN.01170211 pmid: 21885791 |
| [20] |
Zeng CH, Le W, Ni Z, et al. A multicenter application and evaluation of the oxford classification of IgA nephropathy in adult chinese patients[J]. Am J Kidney Dis, 2012,60(5):812-820.
doi: 10.1053/j.ajkd.2012.06.011 URL |
| [21] |
Gutierrez E, Zamora I, Ballarin J A, et al. Long-term outcomes of IgA nephropathy presenting with minimal or no proteinuria[J]. J Am Soc Nephrol, 2012,23(10):1753-1760.
doi: 10.1681/ASN.2012010063 URL |
| [22] |
Wyatt RJ, Julian BA. IgA nephropathy[J]. N Engl J Med, 2013,368(25):2402-2414.
doi: 10.1056/NEJMra1206793 URL |
| [23] |
Fellstrom BC, Barratt J, Cook H, et al. Targeted-release budesonide versus placebo in patients with IgA nephropathy (NEFIGAN): a double-blind, randomised, placebo-controlled phase 2b trial[J]. Lancet, 2017,389(10084):2117-2127.
doi: 10.1016/S0140-6736(17)30550-0 URL |
| [24] |
Inker LA, Mondal H, Greene T, et al. Early change in urine protein as a surrogate end point in studies of IgA nephropathy: An individual-patient meta-analysis[J]. Am J Kidney Dis, 2016,68(3):392-401.
doi: 10.1053/j.ajkd.2016.02.042 URL |
| [1] | Leng Wantong, Tao Jie. Risk factors of postoperative venous thromboembolism in patients with multiple myeloma [J]. Clinical Focus, 2023, 38(4): 340-345. |
| [2] | Wang Jiaoyan, Zhang Yingchun, Ren Keming, Ma Guofeng, Ying Kejing. Clinical analysis of 16 cases of venous thromboembolism combined with psychiatric disorders treated with olanzapine [J]. Clinical Focus, 2022, 37(12): 1108-1113. |
| [3] | Shen Rui, Lei Yanhua, Jia Haokun. Analysis of the incidence and risk factors for venous thromboembolism in 145 patients with diffuse large B-cell lymphoma [J]. Clinical Focus, 2022, 37(1): 43-45. |
| [4] | Xie Changqing, Wang Haifang, Xu Lan, Cai Jianzheng, Zhang Yingying, Yu Weixia. Application value of caprini 2005 risk assessment model in patients with acute stroke [J]. Clinical Focus, 2020, 35(9): 796-800. |
| [5] | Li Tinga, Xu Qiangb, Xing Guangqunc. Analysis of risk factors of thromboembolism in patients with ANCAassociated vasculitis [J]. Clinical Focus, 2019, 34(12): 1098-1101. |
| [6] | Jiang Mingming, Yuan Yadong. Malignant neoplasms and venous thromboembolism [J]. Clinical Focus, 2016, 31(4): 373-377. |
| [7] | Li Hongwei, Wu Qi. Focus on venous thromboembolism during pregnancy [J]. Clinical Focus, 2016, 31(4): 359-362. |
| [8] | Yang Yuanhua, Zhou Rongrong. Progression of diagnosis and treatment in acute pulmonary thromboembolism [J]. Clinical Focus, 2016, 31(4): 349-351. |
| [9] | Qi Shuyuan,Tian Ying. Role of percutaneous left atrial appendage occlusion in stroke prevention for nonvalvular atrial fibrillation [J]. Clinical Focus, 2016, 31(1): 10-13. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||