Clinical Focus ›› 2022, Vol. 37 ›› Issue (3): 234-242.doi: 10.3969/j.issn.1004-583X.2022.03.007
Previous Articles Next Articles
Impact of body mass index in the clinicopathology and prognosis of patients with IgA nephropathy
Gao Pengli, Chen Lili, Tian Fen, Zhang Jiaqian, Chen Yipeng, Qi Xiaojing, Xing Guangqun( )
)
- Department of Nephrology, the Affiliated Hospital of Qingdao University, Qingdao 266555, China
-
Received:2021-09-12Online:2022-03-20Published:2022-04-02 -
Contact:Xing Guangqun E-mail:gqx99monash@163.com
CLC Number:
Cite this article
Gao Pengli, Chen Lili, Tian Fen, Zhang Jiaqian, Chen Yipeng, Qi Xiaojing, Xing Guangqun. Impact of body mass index in the clinicopathology and prognosis of patients with IgA nephropathy[J]. Clinical Focus, 2022, 37(3): 234-242.
share this article
Add to citation manager EndNote|Ris|BibTeX
URL: https://huicui.hebmu.edu.cn/EN/10.3969/j.issn.1004-583X.2022.03.007
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/H值/χ2值 | P值 |
|---|---|---|---|---|---|
| 年龄(岁) | 27.95±8.28 | 38.13±12.71* | 42.4±13.84*# | 14.738 | <0.01 |
| 性别[例(%)] | |||||
| 男 女 | 8(42.2) 11(57.8) | 124(46.4) 143(53.6) | 149(60.3)# 98(39.7)# | 10.810 | <0.01 |
| 收缩压(mmHg) | 119(110, 130) | 130(120, 142)* | 138(130, 150)*# | 45.073 | <0.01 |
| 舒张压(mmHg) | 71(68, 78) | 80(73, 90)* | 83(77, 92)*# | 22.211 | <0.01 |
| 激素或免疫抑制剂治疗[例(%)] | 7(36.8) | 76(28.5) | 73(29.6) | 0.965 | 0.617 |
| ACEI/ARB治疗[例(%)] | 2(10.5) | 110(41.2)* | 138(55.8)*# | 20.098 | <0.01 |
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/H值/χ2值 | P值 |
|---|---|---|---|---|---|
| 年龄(岁) | 27.95±8.28 | 38.13±12.71* | 42.4±13.84*# | 14.738 | <0.01 |
| 性别[例(%)] | |||||
| 男 女 | 8(42.2) 11(57.8) | 124(46.4) 143(53.6) | 149(60.3)# 98(39.7)# | 10.810 | <0.01 |
| 收缩压(mmHg) | 119(110, 130) | 130(120, 142)* | 138(130, 150)*# | 45.073 | <0.01 |
| 舒张压(mmHg) | 71(68, 78) | 80(73, 90)* | 83(77, 92)*# | 22.211 | <0.01 |
| 激素或免疫抑制剂治疗[例(%)] | 7(36.8) | 76(28.5) | 73(29.6) | 0.965 | 0.617 |
| ACEI/ARB治疗[例(%)] | 2(10.5) | 110(41.2)* | 138(55.8)*# | 20.098 | <0.01 |
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | H值/F值 | P值 |
|---|---|---|---|---|---|
| eGFR[ml/(min·1.73 m2)] | 100.3±24.24 | 85.69±30.76* | 80.62±27.72*# | 5.063 | <0.01 |
| 血红蛋白(g/L) | 126.4±20.39 | 128.8±19.74 | 136.7±18.79*# | 11.725 | <0.01 |
| 24小时尿蛋白排泄量(g/d) | 1.38(0.25, 1.98) | 1.13(0.58, 2.26) | 2.01(0.98, 3.55)*# | 35.348 | <0.01 |
| CRP(mg/L) | 1.99(1.15, 3.7) | 1.33(0.79, 2.20) | 1.88(1.05, 3.27)# | 15.372 | <0.01 |
| 中性粒细胞计数(×109/L) | 4.66(3.94, 6.29) | 3.61(2.90, 4.71)* | 3.96(3.14, 4.93) | 12.833 | <0.01 |
| TC(mmol/L) | 4.45(3.36, 5.04) | 4.81(4.17, 5.79) | 4.96(4.21, 6.21) | 5.468 | 0.065 |
| LDL-C(mmol/L) | 2.08(1.45, 2.91) | 2.95(2.41, 3.79)* | 3.14(2.44, 3.98)* | 12.098 | <0.01 |
| BUN(mmol/L) | 4.92(3.93, 6.0) | 5.88(4.60, 7.79) | 5.94(4.60, 7.52) | 4.417 | 0.110 |
| 血UA(μmol/L) | 314.7±102.6 | 354.1±98.88* | 385.40±94.62*# | 9.528 | <0.01 |
| TG(mmol/L) | 0.88(0.60, 1.37) | 1.19(0.88, 1.76) | 1.63(1.16, 2.43)*# | 46.493 | <0.01 |
| CysC(mg/L) | 0.94(0.81, 1.57) | 1.01(0.84, 1.34) | 1.09(0.88, 147) | 3.310 | 0.191 |
| HDL-C(mmol/L) | 1.45(1.22, 1.67) | 1.36(1.16, 1.64) | 1.18(1.02, 1.41)*# | 32.023 | <0.01 |
| FPG(mmol/L) | 4.3(3.99, 4.62) | 4.55(4.25, 4.85) | 4.77(4.34, 5.23)*# | 25.039 | <0.01 |
| 尿红细胞计数(个/μL) | 51(19.1, 109.3) | 65.34(22.8, 132.5) | 56.60(21.12, 117.1) | 1.842 | 0.398 |
| 尿白细胞计数(个/μL) | 5.94(3.5, 16.7) | 7.04(3.96, 13.8) | 6.70(3.30, 14.30) | 0.603 | 0.740 |
| C1q(mg/L) | 167(133.2, 202.3) | 179(155.8, 205.3) | 183(158.9, 205.4) | 3.257 | 0.196 |
| C3(g/L) | 0.88(0.73, 1.03) | 1.01(0.87, 1.14) | 1.12(1.01, 1.28)*# | 54.860 | <0.01 |
| C4(g/L) | 0.22(0.16, 0.26) | 0.23(0.19, 0.28) | 0.27(0.22, 0.32)*# | 29.190 | <0.01 |
| IgG(g/L) | 10.90±3.33 | 10.13±3.49 | 9.99±3.53 | 0.561 | 0.571 |
| IgE(IU/ml) | 59.49(17.16, 155.80) | 66.39(22.67, 149.70) | 50.34(21.93, 141.80) | 0.639 | 0.726 |
| IgA(g/L) | 3.14(2.37, 3.66) | 2.92(2.36, 3.68) | 3.04(2.32, 4.01) | 1.070 | 0.586 |
| IgM(g/L) | 1.04(0.86, 1.58) | 1.00(0.72, 1.41) | 0.89(0.62, 1.25)# | 8.643 | 0.013 |
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | H值/F值 | P值 |
|---|---|---|---|---|---|
| eGFR[ml/(min·1.73 m2)] | 100.3±24.24 | 85.69±30.76* | 80.62±27.72*# | 5.063 | <0.01 |
| 血红蛋白(g/L) | 126.4±20.39 | 128.8±19.74 | 136.7±18.79*# | 11.725 | <0.01 |
| 24小时尿蛋白排泄量(g/d) | 1.38(0.25, 1.98) | 1.13(0.58, 2.26) | 2.01(0.98, 3.55)*# | 35.348 | <0.01 |
| CRP(mg/L) | 1.99(1.15, 3.7) | 1.33(0.79, 2.20) | 1.88(1.05, 3.27)# | 15.372 | <0.01 |
| 中性粒细胞计数(×109/L) | 4.66(3.94, 6.29) | 3.61(2.90, 4.71)* | 3.96(3.14, 4.93) | 12.833 | <0.01 |
| TC(mmol/L) | 4.45(3.36, 5.04) | 4.81(4.17, 5.79) | 4.96(4.21, 6.21) | 5.468 | 0.065 |
| LDL-C(mmol/L) | 2.08(1.45, 2.91) | 2.95(2.41, 3.79)* | 3.14(2.44, 3.98)* | 12.098 | <0.01 |
| BUN(mmol/L) | 4.92(3.93, 6.0) | 5.88(4.60, 7.79) | 5.94(4.60, 7.52) | 4.417 | 0.110 |
| 血UA(μmol/L) | 314.7±102.6 | 354.1±98.88* | 385.40±94.62*# | 9.528 | <0.01 |
| TG(mmol/L) | 0.88(0.60, 1.37) | 1.19(0.88, 1.76) | 1.63(1.16, 2.43)*# | 46.493 | <0.01 |
| CysC(mg/L) | 0.94(0.81, 1.57) | 1.01(0.84, 1.34) | 1.09(0.88, 147) | 3.310 | 0.191 |
| HDL-C(mmol/L) | 1.45(1.22, 1.67) | 1.36(1.16, 1.64) | 1.18(1.02, 1.41)*# | 32.023 | <0.01 |
| FPG(mmol/L) | 4.3(3.99, 4.62) | 4.55(4.25, 4.85) | 4.77(4.34, 5.23)*# | 25.039 | <0.01 |
| 尿红细胞计数(个/μL) | 51(19.1, 109.3) | 65.34(22.8, 132.5) | 56.60(21.12, 117.1) | 1.842 | 0.398 |
| 尿白细胞计数(个/μL) | 5.94(3.5, 16.7) | 7.04(3.96, 13.8) | 6.70(3.30, 14.30) | 0.603 | 0.740 |
| C1q(mg/L) | 167(133.2, 202.3) | 179(155.8, 205.3) | 183(158.9, 205.4) | 3.257 | 0.196 |
| C3(g/L) | 0.88(0.73, 1.03) | 1.01(0.87, 1.14) | 1.12(1.01, 1.28)*# | 54.860 | <0.01 |
| C4(g/L) | 0.22(0.16, 0.26) | 0.23(0.19, 0.28) | 0.27(0.22, 0.32)*# | 29.190 | <0.01 |
| IgG(g/L) | 10.90±3.33 | 10.13±3.49 | 9.99±3.53 | 0.561 | 0.571 |
| IgE(IU/ml) | 59.49(17.16, 155.80) | 66.39(22.67, 149.70) | 50.34(21.93, 141.80) | 0.639 | 0.726 |
| IgA(g/L) | 3.14(2.37, 3.66) | 2.92(2.36, 3.68) | 3.04(2.32, 4.01) | 1.070 | 0.586 |
| IgM(g/L) | 1.04(0.86, 1.58) | 1.00(0.72, 1.41) | 0.89(0.62, 1.25)# | 8.643 | 0.013 |
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/χ2值 | P值 |
|---|---|---|---|---|---|
| 男性 | |||||
| 例数 | 8 | 124 | 149 | ||
| 血红蛋白(g/L) | 126.1±19.25 | 138.9±19.05 | 142.6±16.64* | 4.269 | 0.015 |
| eGFR[ml/(min·1.73 m2)] | 99.56±34.77 | 83.23±32.39 | 79.36±26.61 | 1.947 | 0.145 |
| 血UA(μmol/L) | 382.9±120.7 | 397.6±96.8 | 409.6±95.2 | 0.554 | 0.575 |
| 女性 | |||||
| 例数 | 11 | 143 | 98 | ||
| 血红蛋白(g/L) | 126.5±22.11 | 120.0±15.77 | 127.0±15.55# | 2.711 | <0.01 |
| eGFR[ml/(min·1.73 m2)] | 100.8±14.51 | 87.83±29.23 | 81.96±29.21* | 5.767 | <0.01 |
| 血UA(μmol/L) | 265.2±48.33 | 316.4±84.41 | 350.6±85.42*# | 8.026 | <0.01 |
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/χ2值 | P值 |
|---|---|---|---|---|---|
| 男性 | |||||
| 例数 | 8 | 124 | 149 | ||
| 血红蛋白(g/L) | 126.1±19.25 | 138.9±19.05 | 142.6±16.64* | 4.269 | 0.015 |
| eGFR[ml/(min·1.73 m2)] | 99.56±34.77 | 83.23±32.39 | 79.36±26.61 | 1.947 | 0.145 |
| 血UA(μmol/L) | 382.9±120.7 | 397.6±96.8 | 409.6±95.2 | 0.554 | 0.575 |
| 女性 | |||||
| 例数 | 11 | 143 | 98 | ||
| 血红蛋白(g/L) | 126.5±22.11 | 120.0±15.77 | 127.0±15.55# | 2.711 | <0.01 |
| eGFR[ml/(min·1.73 m2)] | 100.8±14.51 | 87.83±29.23 | 81.96±29.21* | 5.767 | <0.01 |
| 血UA(μmol/L) | 265.2±48.33 | 316.4±84.41 | 350.6±85.42*# | 8.026 | <0.01 |
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/χ2值 | P值 |
|---|---|---|---|---|---|
| 免疫球蛋白沉积强度 | |||||
| IgG | 0.26±0.70 | 0.26±0.67 | 0.33±0.73 | 0.964 | 0.358 |
| IgA | 3.33±0.61 | 3.08±0.79 | 3.05±0.77 | 0.714 | 0.408 |
| IgM | 0.53±0.83 | 0.82±1.02 | 0.79±1.04 | 0.547 | 0.569 |
| 补体沉积强度 | |||||
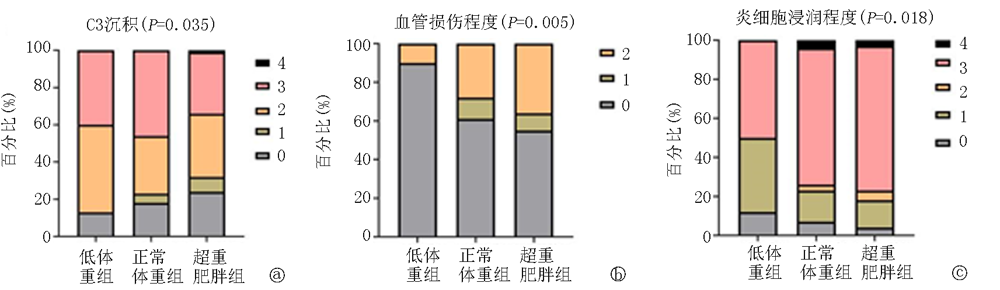
| C3 | 2.13±0.99 | 2.04±1.11 | 1.78±1.18# | 3.848 | 0.035 |
| C1q | 0.14±0.54 | 0.09±0.37 | 0.08±0.36 | 0.422 | 0.615 |
| 炎细胞浸润程度 | 1.88±1.20 | 2.48±1.03* | 2.58±0.91* | 4.068 | 0.018 |
| 血管损伤程度 | 0.26±0.65 | 0.79±0.89* | 0.92±0.95* | 4.947 | 0.007 |
| 牛津病理分型[例(%)] | |||||
| M1 | 14(73.7) | 228(85.4) | 210(85.0) | 1.638 | 0.441 |
| E1 | 3(15.8) | 48(18.0) | 56(22.7) | 3.646 | 0.110 |
| S1 | 7(36.8) | 137(51.3) | 128(51.8) | 1.616 | 0.447 |
| T0 | 16(84.2) | 239(89.5) | 203(82.2) | 5.789 | 0.055 |
| T1+T2 | 3(15.8) | 28(10.5) | 44(17.8) | ||
| C0 | 14(73.7) | 225(84.3) | 215(87.0) | 2.560 | 0.278 |
| C1+C2 | 5(26.3) | 42(15.7) | 32(13.0) |
| 项目 | 低体重组(n=19) | 正常体重组(n=267) | 超重肥胖组(n=247) | F值/χ2值 | P值 |
|---|---|---|---|---|---|
| 免疫球蛋白沉积强度 | |||||
| IgG | 0.26±0.70 | 0.26±0.67 | 0.33±0.73 | 0.964 | 0.358 |
| IgA | 3.33±0.61 | 3.08±0.79 | 3.05±0.77 | 0.714 | 0.408 |
| IgM | 0.53±0.83 | 0.82±1.02 | 0.79±1.04 | 0.547 | 0.569 |
| 补体沉积强度 | |||||
| C3 | 2.13±0.99 | 2.04±1.11 | 1.78±1.18# | 3.848 | 0.035 |
| C1q | 0.14±0.54 | 0.09±0.37 | 0.08±0.36 | 0.422 | 0.615 |
| 炎细胞浸润程度 | 1.88±1.20 | 2.48±1.03* | 2.58±0.91* | 4.068 | 0.018 |
| 血管损伤程度 | 0.26±0.65 | 0.79±0.89* | 0.92±0.95* | 4.947 | 0.007 |
| 牛津病理分型[例(%)] | |||||
| M1 | 14(73.7) | 228(85.4) | 210(85.0) | 1.638 | 0.441 |
| E1 | 3(15.8) | 48(18.0) | 56(22.7) | 3.646 | 0.110 |
| S1 | 7(36.8) | 137(51.3) | 128(51.8) | 1.616 | 0.447 |
| T0 | 16(84.2) | 239(89.5) | 203(82.2) | 5.789 | 0.055 |
| T1+T2 | 3(15.8) | 28(10.5) | 44(17.8) | ||
| C0 | 14(73.7) | 225(84.3) | 215(87.0) | 2.560 | 0.278 |
| C1+C2 | 5(26.3) | 42(15.7) | 32(13.0) |

| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | HR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 年龄 | -0.018 | 0.019 | 0.874 | 0.350 | 0.98 | 0.94 | 1.02 |
| 性别 | 0.561 | 0.499 | 1.262 | 0.261 | 1.75 | 0.66 | 4.66 |
| BMI | 0.136 | 0.077 | 3.115 | 0.049 | 1.17 | 1.00 | 1.36 |
| eGFR | -0.040 | 0.013 | 10.276 | 0.001 | 0.96 | 0.93 | 0.98 |
| 24小时尿蛋白排泄量 | 0.205 | 0.082 | 6.219 | 0.013 | 1.23 | 1.04 | 1.44 |
| 血红蛋白 | -0.042 | 0.011 | 15.790 | 0.000 | 0.96 | 0.94 | 0.98 |
| 血UA | 0.005 | 0.003 | 3.729 | 0.052 | 1.01 | 1.00 | 1.10 |
| TG | 0.275 | 0.135 | 4.125 | 0.042 | 1.32 | 1.01 | 1.72 |
| C3 | 0.510 | 0.946 | 0.291 | 0.573 | 1.79 | 0.23 | 13.86 |
| 肾小管萎缩/间质纤维化比例≥25% | 0.777 | 0.327 | 5.641 | 0.018 | 3.44 | 1.23 | 9.59 |
| 炎细胞浸润程度 | 0.375 | 0.311 | 1.454 | 0.228 | 1.45 | 0.79 | 2.67 |
| 激素和(或)免疫抑制剂治疗 | -0.164 | 0.485 | 0.115 | 0.610 | 0.79 | 0.32 | 1.97 |
| ACEI/ARB治疗 | 0.308 | 0.468 | 0.434 | 0.510 | 1.36 | 0.54 | 3.41 |
| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | HR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 年龄 | -0.018 | 0.019 | 0.874 | 0.350 | 0.98 | 0.94 | 1.02 |
| 性别 | 0.561 | 0.499 | 1.262 | 0.261 | 1.75 | 0.66 | 4.66 |
| BMI | 0.136 | 0.077 | 3.115 | 0.049 | 1.17 | 1.00 | 1.36 |
| eGFR | -0.040 | 0.013 | 10.276 | 0.001 | 0.96 | 0.93 | 0.98 |
| 24小时尿蛋白排泄量 | 0.205 | 0.082 | 6.219 | 0.013 | 1.23 | 1.04 | 1.44 |
| 血红蛋白 | -0.042 | 0.011 | 15.790 | 0.000 | 0.96 | 0.94 | 0.98 |
| 血UA | 0.005 | 0.003 | 3.729 | 0.052 | 1.01 | 1.00 | 1.10 |
| TG | 0.275 | 0.135 | 4.125 | 0.042 | 1.32 | 1.01 | 1.72 |
| C3 | 0.510 | 0.946 | 0.291 | 0.573 | 1.79 | 0.23 | 13.86 |
| 肾小管萎缩/间质纤维化比例≥25% | 0.777 | 0.327 | 5.641 | 0.018 | 3.44 | 1.23 | 9.59 |
| 炎细胞浸润程度 | 0.375 | 0.311 | 1.454 | 0.228 | 1.45 | 0.79 | 2.67 |
| 激素和(或)免疫抑制剂治疗 | -0.164 | 0.485 | 0.115 | 0.610 | 0.79 | 0.32 | 1.97 |
| ACEI/ARB治疗 | 0.308 | 0.468 | 0.434 | 0.510 | 1.36 | 0.54 | 3.41 |
| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | HR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 24小时尿蛋白排泄量 | 0.203 | 0.097 | 4.404 | 0.035 | 1.23 | 1.01 | 1.48 |
| 血红蛋白 | -0.077 | 0.015 | 25.641 | 0.0001 | 0.93 | 0.89 | 0.95 |
| TG | 0.432 | 0.180 | 5.765 | 0.015 | 1.55 | 1.09 | 2.21 |
| 因素 | 回归系数 | 标准误 | Waldχ2值 | P值 | HR值 | 95%CI | |
|---|---|---|---|---|---|---|---|
| 下限 | 上限 | ||||||
| 24小时尿蛋白排泄量 | 0.203 | 0.097 | 4.404 | 0.035 | 1.23 | 1.01 | 1.48 |
| 血红蛋白 | -0.077 | 0.015 | 25.641 | 0.0001 | 0.93 | 0.89 | 0.95 |
| TG | 0.432 | 0.180 | 5.765 | 0.015 | 1.55 | 1.09 | 2.21 |
| [1] |
Rajasekaran A, Julian BA, Rizk DV. IgA nephropathy: An interesting autoimmune kidney disease[J]. Am J Med Sci, 2021, 361(2):176-194.
doi: 10.1016/j.amjms.2020.10.003 pmid: 33309134 |
| [2] |
Roberts IS. Pathology of IgA nephropathy[J]. Nat Rev Nephrol, 2014, 10(8):445-454.
doi: 10.1038/nrneph.2014.92 pmid: 24861083 |
| [3] |
Mohd R, Mohammad Kazmin NE, Abdul Cader R, et al. Long term outcome of immunoglobulin A (IgA) nephropathy: A single center experience[J]. PLoS One, 2021, 16(4):e0249592.
doi: 10.1371/journal.pone.0249592 URL |
| [4] |
Matsuzaki K, Suzuki H, Kawamura T, et al. Utility of remission criteria for the renal prognosis of IgA nephropathy[J]. Clin Exp Nephrol, 2021, 25(9):988-995.
doi: 10.1007/s10157-021-02069-w pmid: 33974158 |
| [5] |
Sagi B, Késõi I, Vas T, et al. The prognostic role of heart rate recovery after exercise and metabolic syndrome in IgA nephropathy[J]. BMC Nephrol, 2021, 22(1):390.
doi: 10.1186/s12882-021-02596-4 URL |
| [6] |
Lu P, Li X, Zhu N, et al. Serum uric acid level is correlated with the clinical, pathological progression and prognosis of IgA nephropathy: An observational retrospective pilot-study[J]. PeerJ, 2020, 8:e10130.
doi: 10.7717/peerj.10130 URL |
| [7] |
Zheng Y, Wang Y, Liu SW, et al. Potential blood pressure goals in IgA nephropathy: Prevalence, awareness, and treatment rates in chronic kidney disease among patients with hypertension in China (PATRIOTIC) study[J]. Kidney Blood Press Res, 2018, 43(6):1786-1795.
doi: 10.1159/000495636 URL |
| [8] |
Zheng W, Mclerran DF, Rolland B, et al. Association between body-mass index and risk of death in more than 1 million Asians[J]. New Engl J Med, 2011, 364(8):719-729.
doi: 10.1056/NEJMoa1010679 URL |
| [9] |
Kataoka H, Ohara M, Shibui K, et al. Overweight and obesity accelerate the progression of IgA nephropathy: Prognostic utility of a combination of BMI and histopathological parameters[J]. Clin Exp Nephrol, 2012, 16(5):706-712.
doi: 10.1007/s10157-012-0613-7 URL |
| [10] |
Wu C, Wang AY, Li G, et al. Association of high body mass index with development of interstitial fibrosis in patients with IgA nephropathy[J]. BMC Nephrol, 2018, 19(1):381.
doi: 10.1186/s12882-018-1164-2 URL |
| [11] |
Ouyang Y, Xie J, Yang M, et al. Underweight is an independent risk factor for renal function deterioration in patients with IgA nephropathy[J]. PLoS One, 2016, 11(9):e0162044.
doi: 10.1371/journal.pone.0162044 URL |
| [12] |
Kikuchi H, Kanda E, Mandai S, et al. Combination of low body mass index and serum albumin level is associated with chronic kidney disease progression: The chronic kidney disease-research of outcomes in treatment and epidemiology (CKD-ROUTE) study[J]. Clin Exp Nephrol, 2017, 21(1):55-62.
doi: 10.1007/s10157-016-1251-2 URL |
| [13] |
Yun HR, Kim H, Park JT, et al. Obesity, metabolic abnormality, and progression of CKD[J]. Am J Kidney Dis, 2018, 72(3):400-410.
doi: 10.1053/j.ajkd.2018.02.362 URL |
| [14] | 裴改琴, 秦嫒雅, 王思清, 等. 血清IgA/C3和病理C3沉积对IgA肾病患者临床预后的影响[J]. 中华医学杂志, 2020, 100(30):2372-2377. |
| [15] |
Jarrick S, Lundberg S, Welander A, et al. Mortality in IgA nephropathy: A nationwide population-based cohort study[J]. J Am Soc Nephrol, 2019, 30(5):866-876.
doi: 10.1681/ASN.2018101017 pmid: 30971457 |
| [16] |
Wang Y, Zhao L, Gao L, et al. Health policy and public health implications of obesity in China[J]. Lancet Diabetes Endocrinol, 2021, 9(7):446-461.
doi: 10.1016/S2213-8587(21)00118-2 URL |
| [17] |
Pan XF, Wang LM, Pan A. Epidemiology and determinants of obesity in China[J]. Lancet Diabetes Endocrinol, 2021, 9(6):373-392.
doi: 10.1016/S2213-8587(21)00045-0 URL |
| [18] |
Lai YJ, Hu HY, Lee YL, et al. Association between obesity and risk of chronic kidney disease: A nationwide cohort study in Taiwan[J]. Nutr Metab Cardiovasc Dis, 2017, 27(11):1008-1014.
doi: S0939-4753(17)30200-4 pmid: 28986076 |
| [19] |
Wang Y, Chen X, Song Y, et al. Association between obesity and kidney disease: A systematic review and meta-analysis[J]. Kidney Int, 2008, 73(1):19-33.
pmid: 17928825 |
| [20] |
Zoccali C. The obesity epidemics in ESRD: From wasting to waist?[J]. Nephrol Dial Transplant, 2009, 24(2):376-380.
doi: 10.1093/ndt/gfn589 URL |
| [21] |
Berthoux F, Mohey H, Laurent B, et al. Predicting the risk for dialysis or death in IgA nephropathy[J]. J Am Soc Nephrol, 2011, 22(4):752-761.
doi: 10.1681/ASN.2010040355 URL |
| [22] |
Choi WJ, Hong YA, Min JW, et al. The serum uric acid level is related to the more severe renal histopathology of female IgA nephropathy patients[J]. J Clin Med, 2021, 10(9) : 1885.
doi: 10.3390/jcm10091885 URL |
| [23] |
Yonekura Y, Goto S, Sugiyama H, et al. The influences of larger physical constitutions including obesity on the amount of urine protein excretion in primary glomerulonephritis: Research of the Japan renal biopsy registry[J]. Clin Exp Nephrol, 2015, 19(3):359-370.
doi: 10.1007/s10157-014-0993-y pmid: 24916004 |
| [24] |
Fox CS, Larson MG, Leip EP, et al. Predictors of new-onset kidney disease in a community-based population[J]. JAMA, 2004, 291(7):844-850.
doi: 10.1001/jama.291.7.844 URL |
| [25] |
Kalaitzidis RG, Siamopoulos KC. The role of obesity in kidney disease: Recent findings and potential mechanisms[J]. Int Urol Nephrol, 2011, 43(3):771-784.
doi: 10.1007/s11255-011-9974-1 pmid: 21544651 |
| [26] |
Tanaka M, Yamada S, Iwasaki Y, et al. Impact of obesity on IgA nephropathy: Comparative ultrastructural study between obese and non-obese patients[J]. Nephron Clin Pract, 2009, 112(2):c71-c78.
doi: 10.1159/000213084 URL |
| [27] |
Gabrielsson BG, Johansson JM, Lonn M, et al. High expression of complement components in omental adipose tissue in obese men[J]. Obes Res, 2003, 11(6):699-708.
pmid: 12805391 |
| [28] |
Karkhaneh M, Qorbani M, Mohajeri-Tehrani MR, et al. Association of serum complement C3 with metabolic syndrome components in normal weight obese women[J]. J Diabetes Metab Disord, 2017, 16:49.
doi: 10.1186/s40200-017-0330-6 URL |
| [29] |
Ohsawa I, Inoshita H, Ishii M, et al. Metabolic impact on serum levels of complement component 3 in Japanese patients[J]. J Clin Lab Anal, 2010, 24(2):113-118.
doi: 10.1002/jcla.20372 pmid: 20333766 |
| [30] |
Wlazlo N, van Greevenbroek MM, Ferreira I, et al. Low-grade inflammation and insulin resistance independently explain substantial parts of the association between body fat and serum C3: The CODAM study[J]. Metabolism, 2012, 61(12):1787-1796.
doi: 10.1016/j.metabol.2012.05.015 URL |
| [31] |
Al Haj Ahmad RM, Al-Domi HA. Complement 3 serum levels as a pro-inflammatory biomarker for insulin resistance in obesity[J]. Diabetes Metab Syndr, 2017, 11:S229-S232.
doi: 10.1016/j.dsx.2016.12.036 URL |
| [32] |
Engstrom G, Hedblad B, Janzon L, et al. Weight gain in relation to plasma levels of complement factor 3: Results from a population-based cohort study[J]. Diabetologia, 2005, 48(12):2525-2531.
doi: 10.1007/s00125-005-0021-6 URL |
| [33] |
Harmon DB, Srikakulapu P, Kaplan JL, et al. Protective role for B-1b B cells and IgM in obesity-associated inflammation, glucose intolerance, and insulin resistance[J]. Arterioscler Thromb Vasc Biol, 2016, 36(4):682-691.
doi: 10.1161/ATVBAHA.116.307166 URL |
| [34] |
Stefan G, Ismail G, Stancu S, et al. Validation study of Oxford classification of IgA nephropathy: The significance of extracapillary hypercellularity and mesangial IgG immunostaining[J]. Pathol Int, 2016, 66(8):453-459.
doi: 10.1111/pin.2016.66.issue-8 URL |
| [35] |
Hong YA, Min JW, Ha MA, et al. The impact of obesity on the severity of clinicopathologic parameters in patients with IgA nephropathy[J]. J Clin Med, 2020, 9(9) : 2824.
doi: 10.3390/jcm9092824 URL |
| [36] |
Nam KH, Joo YS, Lee C, et al. Predictive value of mesangial C3 and C4d deposition in IgA nephropathy[J]. Clin Immunol, 2020, 211:108331.
doi: 10.1016/j.clim.2019.108331 URL |
| [37] |
Park S, Kim HW, Park JT, et al. Relationship between complement deposition and the Oxford classification score and their combined effects on renal outcome in immunoglobulin A nephropathy[J]. Nephrol Dial Transplant, 2020, 35(12):2103-2137.
doi: 10.1093/ndt/gfz179 URL |
| [38] |
Lee H, Kim DK, Oh KH, et al. Mortality of IgA nephropathy patients: A single center experience over 30 years[J]. PLoS One, 2012, 7(12):e51225.
doi: 10.1371/journal.pone.0051225 URL |
| [39] |
Le W, Liang S, Hu Y, et al. Long-term renal survival and related risk factors in patients with IgA nephropathy: Results from a cohort of 1155 cases in a Chinese adult population[J]. Nephrol Dial Transpl, 2012, 27(4):1479-1485.
doi: 10.1093/ndt/gfr527 URL |
| [40] |
Praga M, Morales E. Obesity, proteinuria and progression of renal failure[J]. Curr Opin Nephrol Hypertens, 2006, 15(5):481-486.
doi: 10.1097/01.mnh.0000242172.06459.7c URL |
| [41] |
Al-Hashem FH. Is it necessary to consider obesity when constructing norms for hemoglobin or when screening for anemia using hemoglobin levels?[J]. Saudi Med J, 2007, 28(1):41-45.
pmid: 17206287 |
| [42] |
Theodore B. Health implications of overweight and obesity in the United States[J]. Ann Intern Med, 1985, 103:983-988.
doi: 10.7326/0003-4819-103-6-983 URL |
| [43] |
Oh TR, Song SH, Choi HS, et al. The association between serum hemoglobin and renal prognosis of IgA nephropathy[J]. J Clin Med, 2021, 10(2):363.
doi: 10.3390/jcm10020363 URL |
| [44] |
Zhu B, Liu WH, Yu DR, et al. The association of low hemoglobin levels with IgA nephropathy progression: A two-center cohort study of 1, 828 cases[J]. Am J Nephrol, 2020, 51(8):624-634.
doi: 10.1159/000508770 URL |
| [45] |
van Iterson EH, Kim CH, Uithoven K, et al. Obesity and hemoglobin content impact peak oxygen uptake in human heart failure[J]. Eur J Prev Cardiol, 2018, 25(18):1937-1946.
doi: 10.1177/2047487318802695 pmid: 30247068 |
| [1] | Liu Lili, Yuan Yuting, Lai Gengliang, Tian Chuan, Lan Xiang, Ye Zhonglv. The relationship between minimal residual disease on day 15 and prognosis in children with acute lymphoblastic leukemia [J]. Clinical Focus, 2024, 39(1): 47-52. |
| [2] | Wang Tao, Gao Yuwei, Wang Xinghua, Hu Xiuhong, Cui Hongrui, Xu Baozhen, Yang Hongjuan. Correlation of anti-phospholipase A2 receptor antibody with idiopathic membranous nephropathy [J]. Clinical Focus, 2023, 38(7): 606-612. |
| [3] | Gao Qinyu, Bao Beiyan, Jin Yan, Zhao Yu. Analysis of clinical features and prognostic factors of IgA nephropathy complicated with depression [J]. Clinical Focus, 2023, 38(6): 510-515. |
| [4] | Sun Xingxing, Lin Hai. Changes in immune function and prognostic risk factors for severe pneumonia in children [J]. Clinical Focus, 2023, 38(6): 521-525. |
| [5] | Liu Jing, Luo Na, Feng Shangyong, Wang Yan, Zhang Zhenwen, She Dunmin. Prevalence and risk factors of hyperuricemia in health examination population in Yangzhou, 2020 [J]. Clinical Focus, 2023, 38(5): 428-432. |
| [6] | He Xiangyu, Pan Yan, Zhang Xiaolin. Correlation between serum lipoprotein-associated phospholipase A2 level and the severity and prognosis of acute ischemic stroke [J]. Clinical Focus, 2023, 38(4): 315-318. |
| [7] | Yang Jinqiang, Zhang Renmin. Prognostic value of procalcitonin to platelet ratio in patients with fever with thrombocytopenia syndrome [J]. Clinical Focus, 2023, 38(4): 346-351. |
| [8] | Luo Jie, Wu Qiang, Li Zhong, Zheng Shuo. Rare adrenal neurofibroma: A case report and literature review [J]. Clinical Focus, 2023, 38(4): 359-363. |
| [9] | Zhang Na, Sun Yue, Dong Han, Zhao Peng, Yang Xin, Qi Yuan, Wang Lingling. Correlation between the expression level of SPARC and prognosis in patients with non-small cell lung cancer: A meta-analysis [J]. Clinical Focus, 2023, 38(11): 972-978. |
| [10] | He Peihua, Zhou Xingfu, Hong Weihong, Wang Lichun, Liu Sujun, Jin Yuyan, Zeng Jiahao, Liu Lichang. Clinical analysis of 4 cases of IgG4-related kidney disease [J]. Clinical Focus, 2023, 38(11): 1016-1021. |
| [11] | Liu Ye, Ruan Guiren, Liu Xiaoqing, Shi Xiaochun, Fei Guijun. Diagnosis and differential diagnosis of pancreatic tuberculosis [J]. Clinical Focus, 2023, 38(10): 898-903. |
| [12] | Wang Huixin, Zhao Fangqing, Zhang Xinyan, Hou Xiaowen. Relationship between uric acid and prognosis of Chinese patients with acute ischemic stroke: A meta analysis [J]. Clinical Focus, 2022, 37(9): 785-790. |
| [13] | Zhou Bin, Zeng Cizheng, Huang Yuge, Zhong Mianling, Wu Jiayuan. Effect of pSOFA score combined with C-reactive protein and procalcitonin in prognosis assessment of sepsis children [J]. Clinical Focus, 2022, 37(7): 616-622. |
| [14] | Ye Qian, Ling Zhai, Liu Shenxiang, Lu Guotao, Yin Xudong. Meta analysis on effects of glucocorticoid on the immunotherapy of advanced cancer [J]. Clinical Focus, 2022, 37(7): 591-598. |
| [15] | Zhang Mengyuan, Zhu Yong. Predictive value of procalcitonin clearance and SOFA score on the prognosis of patients with severe sepsis [J]. Clinical Focus, 2022, 37(3): 225-229. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||