Clinical Focus ›› 2023, Vol. 38 ›› Issue (11): 1016-1021.doi: 10.3969/j.issn.1004-583X.2023.11.010
Previous Articles Next Articles
Clinical analysis of 4 cases of IgG4-related kidney disease
He Peihua1, Zhou Xingfu1, Hong Weihong2, Wang Lichun2, Liu Sujun2, Jin Yuyan2, Zeng Jiahao2, Liu Lichang2( )
)
- 1. The Second Clinical MedicalCol lege of Guangzhou University of Chinese Medicine, Guangzhou 510006,China
2. Department of Nephrology, Guangdong Provincial Hospital of Chinese Medicine,Zhuhai,Zhuhai 519015,China
-
Received:2023-01-19Online:2023-11-20Published:2024-01-17 -
Contact:Liu Lichang E-mail:1225929054@qq.com
CLC Number:
Cite this article
He Peihua, Zhou Xingfu, Hong Weihong, Wang Lichun, Liu Sujun, Jin Yuyan, Zeng Jiahao, Liu Lichang. Clinical analysis of 4 cases of IgG4-related kidney disease[J]. Clinical Focus, 2023, 38(11): 1016-1021.
share this article
Add to citation manager EndNote|Ris|BibTeX
URL: https://huicui.hebmu.edu.cn/EN/10.3969/j.issn.1004-583X.2023.11.010
| 病例 | 年龄(岁) | 性别 | 病程(月) | 主要症状 | 体格检查 | 受累器官 |
|---|---|---|---|---|---|---|
| 患者1 | 76 | 男 | 1 | 乏力、纳差、少尿至无尿 | 左下肢轻度凹陷性浮肿 | 肾脏 |
| 患者2 | 66 | 女 | 1 | 乏力、纳差 | 无特殊 | 肾脏 |
| 患者3 | 88 | 男 | 48 | 乏力、纳差、腹痛 | 双足背轻度凹陷性浮肿 | 肾脏、胰腺 |
| 患者4 | 56 | 男 | 9 | 乏力、纳差、恶心呕吐 | 左下肢轻度凹陷性浮肿 | 肾脏、腹膜后 |
Tab.1 General information and clinical manifestations
| 病例 | 年龄(岁) | 性别 | 病程(月) | 主要症状 | 体格检查 | 受累器官 |
|---|---|---|---|---|---|---|
| 患者1 | 76 | 男 | 1 | 乏力、纳差、少尿至无尿 | 左下肢轻度凹陷性浮肿 | 肾脏 |
| 患者2 | 66 | 女 | 1 | 乏力、纳差 | 无特殊 | 肾脏 |
| 患者3 | 88 | 男 | 48 | 乏力、纳差、腹痛 | 双足背轻度凹陷性浮肿 | 肾脏、胰腺 |
| 患者4 | 56 | 男 | 9 | 乏力、纳差、恶心呕吐 | 左下肢轻度凹陷性浮肿 | 肾脏、腹膜后 |
| 病例 | 血清肌酐 (58.0~110.0 μmol/L) | 血清IgG (8.00~17.00 g/L) | 血清IgG4 (0.08~1.35 g/L) | 补体3 (0.90~1.80 g/L) | 补体4 (0.10~0.40 g/L) | 尿微量白蛋白 (0.0~20.0 mg/L) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 患者1 | 1 503.1 | 16.96 | NA | 0.63 | 0.16 | 146.4 | |||||
| 患者2 | 271.0 | 23.1 | 3.09 | 1.52 | 0.48 | NA | |||||
| 患者3 | 129.1 | 23.03 | 3.20 | 1.67 | 0.41 | 19.0 | |||||
| 患者4 | 1 448.6 | 22.42 | 3.00 | 0.40 | 0.07 | 59.6 | |||||
| 患者 | 尿β2微球蛋白 (0.11~0.32 mg/L) | 24h尿蛋白总量 (mg/24h) (<150 mg/24h) | 血清白蛋白 (40.0~55.0 g/L) | 血红蛋白 (130~175 g/L) | 血清淀粉酶 (35.0~135.0 U/L) | 血清脂肪酶 (23.0~300.0 U/L) | |||||
| 患者1 | 7.79 | NA | 30.3 | 85 | 84.0 | NA | |||||
| 患者2 | NA | 1277.65 | 39.5 | 108 | NA | NA | |||||
| 患者3 | 0.55 | 191.31 | 31.0 | 99 | 316.0 | 1274.5 | |||||
| 患者4 | 10.30 | 1400.64 | 35.8 | 96 | 172.7 | 478.2 | |||||
Tab. 2 Laboratory inspection
| 病例 | 血清肌酐 (58.0~110.0 μmol/L) | 血清IgG (8.00~17.00 g/L) | 血清IgG4 (0.08~1.35 g/L) | 补体3 (0.90~1.80 g/L) | 补体4 (0.10~0.40 g/L) | 尿微量白蛋白 (0.0~20.0 mg/L) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 患者1 | 1 503.1 | 16.96 | NA | 0.63 | 0.16 | 146.4 | |||||
| 患者2 | 271.0 | 23.1 | 3.09 | 1.52 | 0.48 | NA | |||||
| 患者3 | 129.1 | 23.03 | 3.20 | 1.67 | 0.41 | 19.0 | |||||
| 患者4 | 1 448.6 | 22.42 | 3.00 | 0.40 | 0.07 | 59.6 | |||||
| 患者 | 尿β2微球蛋白 (0.11~0.32 mg/L) | 24h尿蛋白总量 (mg/24h) (<150 mg/24h) | 血清白蛋白 (40.0~55.0 g/L) | 血红蛋白 (130~175 g/L) | 血清淀粉酶 (35.0~135.0 U/L) | 血清脂肪酶 (23.0~300.0 U/L) | |||||
| 患者1 | 7.79 | NA | 30.3 | 85 | 84.0 | NA | |||||
| 患者2 | NA | 1277.65 | 39.5 | 108 | NA | NA | |||||
| 患者3 | 0.55 | 191.31 | 31.0 | 99 | 316.0 | 1274.5 | |||||
| 患者4 | 10.30 | 1400.64 | 35.8 | 96 | 172.7 | 478.2 | |||||
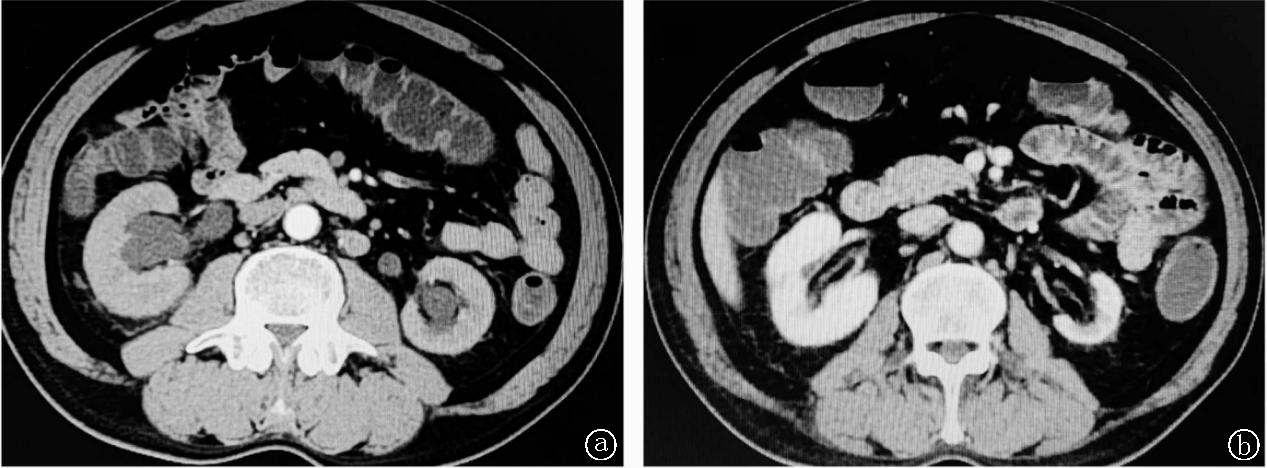
Fig.1 Abdominal enhanced CT of patients 3 a. before treatment; b.after treatment
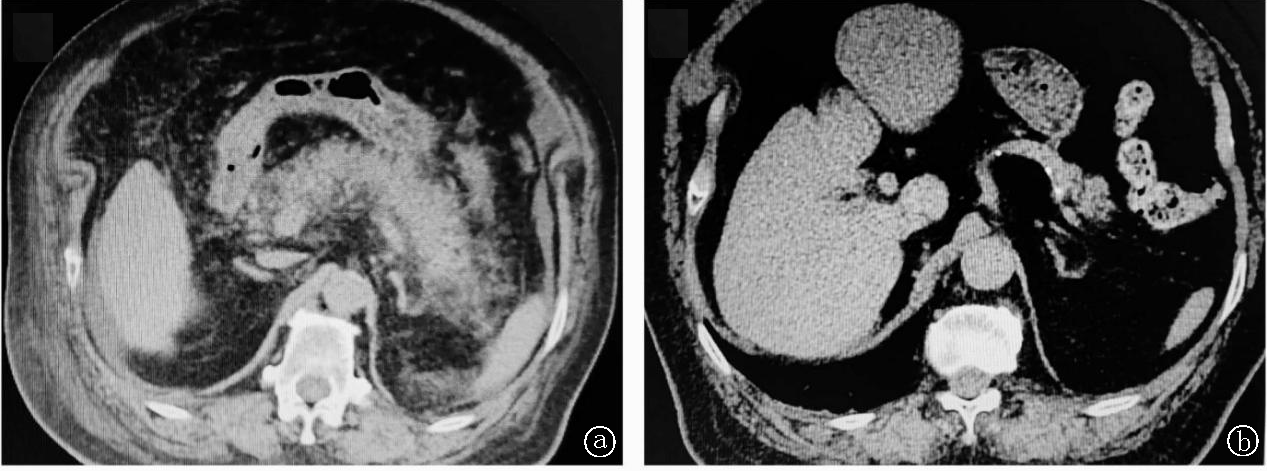
Fig.2 Abdominal enhanced CT of patients 4 a. before treatment; b.after treatment
| 肾脏病理 | 患者1 | 患者2 | 患者3 | 患者4 |
|---|---|---|---|---|
| 光镜 | ||||
| 肾小球总数(个) | 5 | 20 | 10 | 3 |
| 肾小球病变(个) | 0 | 0 | 2 | 1 |
| 肾间质病变 | ||||
| 肾间质纤维化 | 灶状 | 灶状 | 鸟眼状 | 灶状 |
| 炎症细胞浸润 | 弥漫性 | 弥漫性 | 弥漫性 | 弥漫性 |
| 肾小管萎缩 | 部分 | 无 | 灶状(萎缩面积>30%) | 灶状(萎缩面积>10%) |
| 免疫荧光 | IgM+ | IgM+ | IgM+ | 无 |
| 免疫组化 | 部分浆细胞IgG4染色阳性 | IgG4/IgG<40%,IgG4阳性细胞数局灶区域>10/HPF | IgG4/IgG<40%,IgG4阳性细胞数局灶区域>10/HPF | IgG4/IgG>40%,IgG4阳性细胞数局灶区域>10/HPF |
| 电镜 | ||||
| 电子致密物沉积 | 无 | 无 | 无 | 无 |
| 诊断 | IgG4-TIN | IgG4-TIN | IgG4-TIN | IgG4-TIN |
Tab.3 Renal pathological results
| 肾脏病理 | 患者1 | 患者2 | 患者3 | 患者4 |
|---|---|---|---|---|
| 光镜 | ||||
| 肾小球总数(个) | 5 | 20 | 10 | 3 |
| 肾小球病变(个) | 0 | 0 | 2 | 1 |
| 肾间质病变 | ||||
| 肾间质纤维化 | 灶状 | 灶状 | 鸟眼状 | 灶状 |
| 炎症细胞浸润 | 弥漫性 | 弥漫性 | 弥漫性 | 弥漫性 |
| 肾小管萎缩 | 部分 | 无 | 灶状(萎缩面积>30%) | 灶状(萎缩面积>10%) |
| 免疫荧光 | IgM+ | IgM+ | IgM+ | 无 |
| 免疫组化 | 部分浆细胞IgG4染色阳性 | IgG4/IgG<40%,IgG4阳性细胞数局灶区域>10/HPF | IgG4/IgG<40%,IgG4阳性细胞数局灶区域>10/HPF | IgG4/IgG>40%,IgG4阳性细胞数局灶区域>10/HPF |
| 电镜 | ||||
| 电子致密物沉积 | 无 | 无 | 无 | 无 |
| 诊断 | IgG4-TIN | IgG4-TIN | IgG4-TIN | IgG4-TIN |
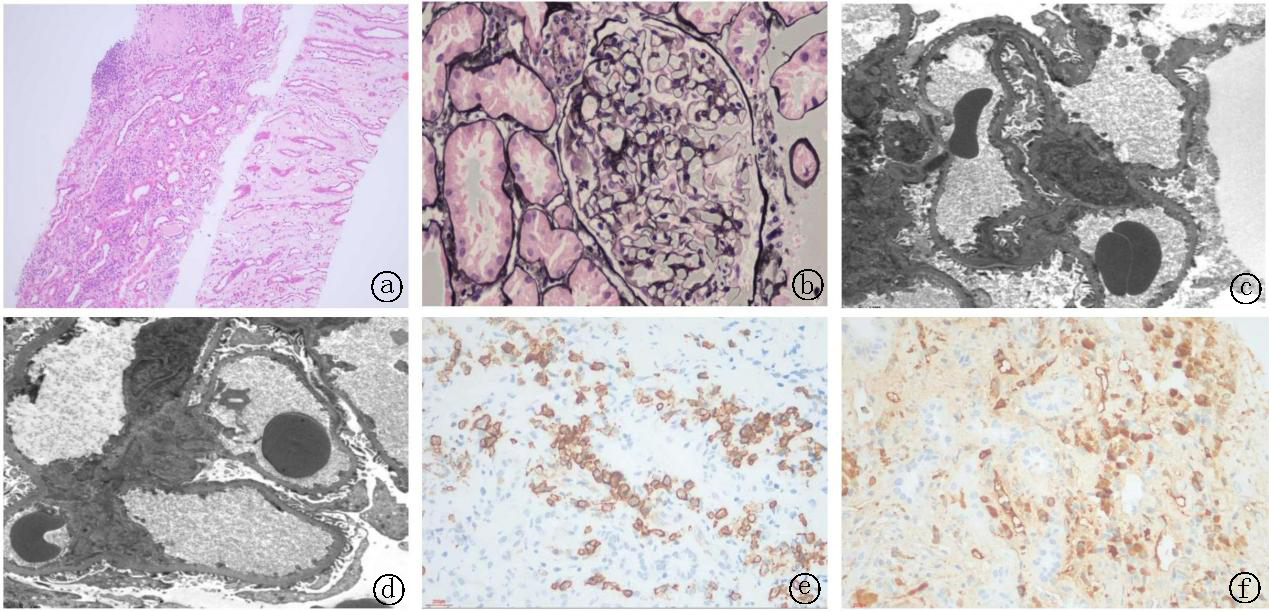
Fig.3 Typical renal pathological changes a~b. light microscopy (HE stain): It could see focal or bird eye fibrosis (a), the renal interstitium was infiltrated by focal inflammatory cell and bird eye fibrosis, which could see plasma cells (b); c~d. electron microscopy: No obvious depoasis were observed. e~f. Immunohistochemistry: There were CD38-positive plasma cells and CD138-positive plasma cells(e); there were many IgG4 plasma cells and they were over 10/HPF (f)
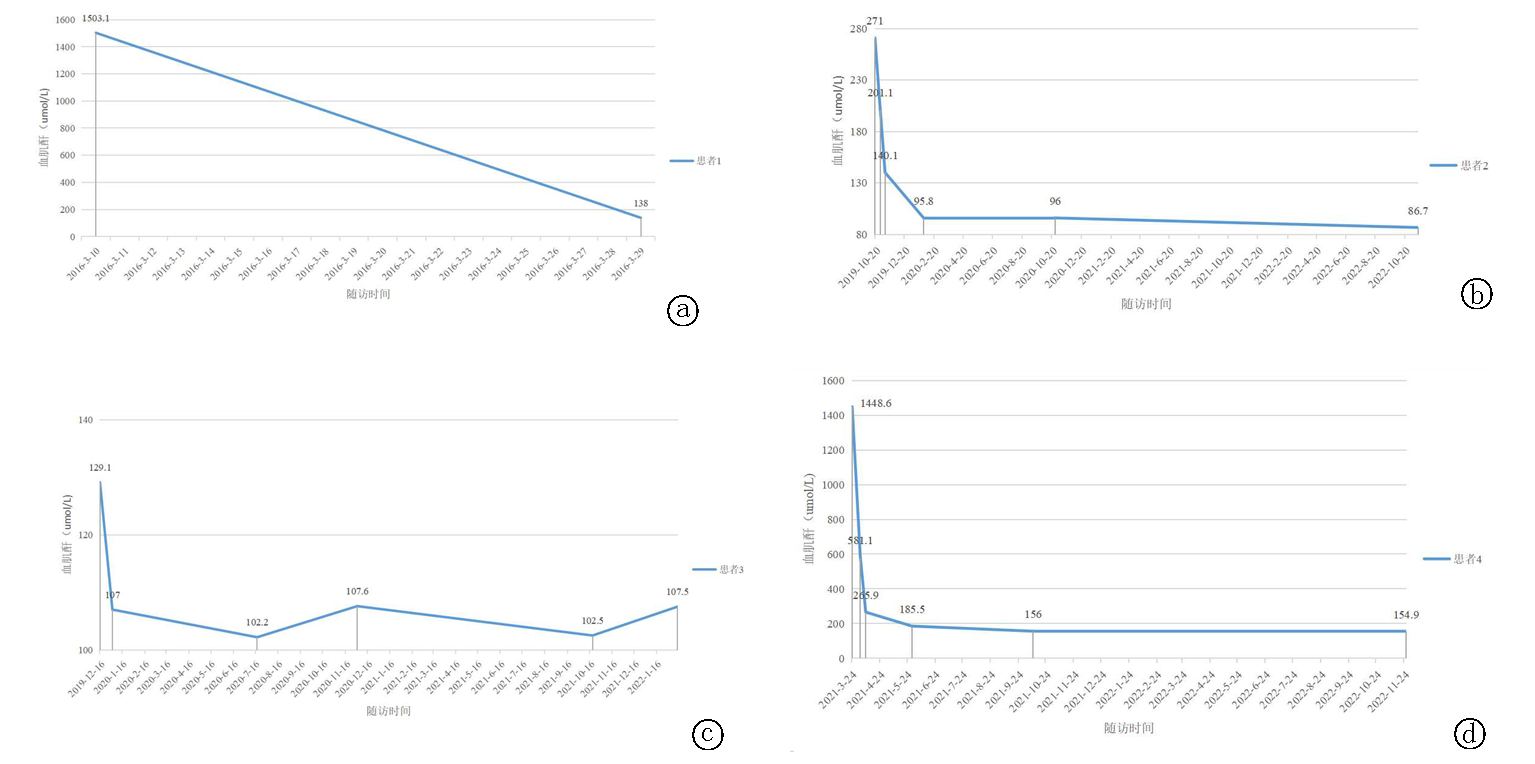
Fig.4 Changes in blood creatinine levels a. patient 1; b. patient 2; c. patient 3; d. patient 4
| [1] |
Umehara H, Okazaki K, Masaki Y, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011[J]. Mod Rheumatol, 2012, 22(1):21-30.
doi: 10.1007/s10165-011-0571-z pmid: 22218969 |
| [2] | 高丽霞. IgG4相关性疾病的诊治及进展[J]. 临床荟萃, 2016, 31(5):501-505. |
| [3] |
Yoshida K, Toki F, Takeuchi T, et al. Chronic pancreatitis caused by an autoimmune abnormality. Proposal of the concept of autoimmune pancreatitis[J]. Dig Dis Sci, 1995, 40(7):1561-1568.
doi: 10.1007/BF02285209 URL |
| [4] |
Takahashi H, Yamamoto M, Suzuki C, et al. The birthday of a new syndrome: IgG4-related diseases constitute a clinical entity[J]. Autoimmun Rev, 2010, 9(9):591-594.
doi: 10.1016/j.autrev.2010.05.003 pmid: 20457280 |
| [5] |
Boffa JJ, Esteve E, Buob D. Renal involvement in IgG4-related disease[J]. Presse Med, 2020, 49(1):104017.
doi: 10.1016/j.lpm.2020.104017 URL |
| [6] |
Nakashima H, Kawano M, Saeki T, et al. Estimation of the number of histological diagnosis for IgG4-related kidney disease referred to the data obtained from the Japan Renal Biopsy Registry (J-RBR) questionnaire and cases reported in the Japanese Society of Nephrology Meetings[J]. Clin Exp Nephrol, 2017, 21(1):97-103.
doi: 10.1007/s10157-016-1260-1 pmid: 27015831 |
| [7] |
Raissian Y, Nasr SH, Larsen CP, et al. Diagnosis of IgG4-related tubulointerstitial nephritis[J]. J Am Soc Nephrol, 2011, 22(7):1343-1352.
doi: 10.1681/ASN.2011010062 pmid: 21719792 |
| [8] |
Saeki T, Nishi S, Imai N, et al. Clinicopathological characteristics of patients with IgG4-related tubulointerstitial nephritis[J]. Kidney Int, 2010, 78(10):1016-1023.
doi: 10.1038/ki.2010.271 pmid: 20720530 |
| [9] |
Jain K, Sengupta M, Basu K, et al. IgG4 tubulointerstitial nephritis-An uncommon enemy![J]. Indian J Pathol Microbiol, 2021, 64(3):556-558.
doi: 10.4103/IJPM.IJPM_687_20 URL |
| [10] | 揭淇, 徐嘉琪, 雷莹, 等. IgG4相关性间质性肾炎一例报告并文献复习[J]. 国际移植与血液净化杂志, 2021, 19(3):27-29. |
| [11] | 李娟, 沈淑琼, 许树根, 等. IgG4相关性肾病一例[J]. 中华肾脏病杂志, 2011, 27(10):794. |
| [12] | 汪志祥, 陈文莉, 裴广畅, 等. IgG4相关性肾小管间质肾炎一例报告[J]. 临床肾脏病杂志, 2014, 14(3):192-193. |
| [13] | 陈欣, 刘红, 金是, 等. IgG4相关性肾病2例报告[J]. 中国临床医学, 2021, 28(6):1092-1097. |
| [14] |
Kawano M, Saeki T, Nakashima H. IgG4-related kidney disease and retroperitoneal fibrosis: An update[J]. Mod Rheumatol, 2019, 29(2):231-239.
doi: 10.1080/14397595.2018.1554321 pmid: 30499730 |
| [15] |
Evans R, Cargill T, Goodchild G, et al. Clinical manifestations and long-term outcomes of IgG4-related kidney and retroperitoneal involvement in a United Kingdom IgG4-related disease cohort[J]. Kidney Int Rep, 2019, 4(1):48-58.
doi: 10.1016/j.ekir.2018.08.011 pmid: 30596168 |
| [16] | 雒真龙, 潘昊, 裴广畅, 等. IgG4相关性疾病伴肾脏损害病例报告并文献复习[J]. 内科急危重症杂志, 2015, 21(6):419-422, 425. |
| [17] | 王红月, 石海菊, 罗莉娟, 等. 糖尿病合并IgG4相关性疾病伴肾功能不全一例[J]. 中华全科医师杂志, 2021, 20(2):236-238. |
| [18] | 李聚敏, 周焕芝, 邹万忠, 等. IgA肾病伴IgG4相关性间质性肾炎1例报道[J]. 解放军医学杂志, 2014, 39(7):590-592. |
| [19] | 尹清, 刘必成. 以急性肾衰竭为主要表现的腹膜后纤维化1例并文献复习[J]. 临床荟萃, 2017, 32(8):717-721. |
| [20] | 曹伟华, 常娟锋, 蒋立明. 腹膜后纤维化的CT诊断及误诊分析[J]. 现代医用影像学, 2022, 31(6):1010-1014. |
| [21] |
Takeda S, Haratake J, Kasai T, et al. IgG4-associated idiopathic tubulointerstitial nephritis complicating autoimmune pancreatitis[J]. Nephrol Dial Transplant, 2004, 19(2):474-476.
doi: 10.1093/ndt/gfg477 URL |
| [22] | 王佳妮, 靳二虎. 影像学诊断及鉴别诊断自身免疫性胰腺炎[J]. 中国医学影像技术, 2021, 37(7):1102-1105. |
| [23] | 丁航, 刘源, 张连峰, 等. 血清IgG4对IgG4相关性疾病诊断价值的Meta分析[J]. 临床荟萃, 2021, 36(7):587-594. |
| [24] |
Wang R, He D, Zhao L, et al. Role of complement system in patients with biopsy-proven immunoglobulin G4-related kidney disease[J]. Hum Pathol, 2018, 81:220-228.
doi: S0046-8177(18)30266-1 pmid: 30031099 |
| [25] | 王荣, 何大锋, 鲁春苗, 等. 补体系统在IgG4相关性肾病中的临床意义[J]. 中华临床免疫和变态反应杂志, 2022, 16(4):368-376. |
| [26] |
Wu H, Wang C, Woywodt A, et al. Concurrent presentation of IgG4-related tubulointerstitial nephritis and ANCA MPO crescentic glomerulonephritis[J]. Clin Nephrol Case Stud, 2022, 10:47-53.
doi: 10.5414/CNCS110852 pmid: 35837351 |
| [27] |
Faz-Muñoz D, Hinojosa-Azaola A, Mejía-Vilet JM, et al. ANCA-associated vasculitis and IgG4-related disease overlap syndrome: A case report and literature review[J]. Immunol Res, 2022, 70(4):550-559.
doi: 10.1007/s12026-022-09279-8 |
| [28] |
Kawano M, Saeki T, Nakashima H, et al. Proposal for diagnostic criteria for IgG4-related kidney disease[J]. Clin Exp Nephrol, 2011, 15(5):615-626.
doi: 10.1007/s10157-011-0521-2 pmid: 21898030 |
| [29] |
邱亚桂, 夏茜, 陈雁扬, 等. IgG4相关慢性间质性肾炎并肾包膜纤维化一例报告暨文献复习[J]. 中华肾脏病杂志, 2019, 35(11):822-827.
doi: 10.3760/cma.j.issn.1001-7097.2019.11.004 |
| [30] | 邓文友, 郭小芳, 闫卫鹏, 等. IgG4相关性肾病伴双侧肾盂损害1例[J]. 中国医学影像技术, 2019, 35(12):1918-1919. |
| [31] | Wallace ZS, Naden RP, Chari S, et al. The 2019 American College of Rheumatology/European League Against Rheumatism classification criteria for IgG4-related disease[J]. Ann Rheum Dis, 2020, 79(1):77-87. |
| [32] |
Khosroshahi A, Wallace ZS, Crowe JL, et al. International consensus guidance statement on the management and treatment of IgG4-related disease[J]. Arthritis Rheumatol, 2015, 67(7):1688-1699.
doi: 10.1002/art.v67.7 URL |
| [33] | 孙响波. 黑地黄丸治疗IgG4相关性间质性肾炎1例报告[J]. 中国中西医结合肾病杂志, 2017, 18(2):160-161. |
| [1] | Song Jialiang, Jiang Yingjie, Kong Ruina, Cai Qing, Gao Jie. IgG4-related diseases characterized by increased IgE level and eosinophil count with multiple lymphadenopathy: A case report [J]. Clinical Focus, 2024, 39(1): 57-60. |
| [2] | Li Yang, Mo Feng, Xin Zhifei, Wang Qian, Deng Xinna. Multiple immune related adverse events with special clinical manifestations: A case report [J]. Clinical Focus, 2023, 38(7): 633-637. |
| [3] | Xiao Meng, Cheng Tingting, Ma Qiange, Feng Xiaoying, Li Lihua, Li Tao. Clinical characteristics and laboratory examination of Epstein-Barr virus infection and infectious mononucleosis in Chengde [J]. Clinical Focus, 2023, 38(6): 526-531. |
| [4] | Lin Changyi, Song Minghui, Wu Peicheng. Effects of diagnosis age on clinical manifestations of polymyalgia rheumatica: A single center retrospective cohort study on 68 patients [J]. Clinical Focus, 2022, 37(7): 612-615. |
| [5] | Ye Qian, Ling Zhai, Liu Shenxiang, Lu Guotao, Yin Xudong. Meta analysis on effects of glucocorticoid on the immunotherapy of advanced cancer [J]. Clinical Focus, 2022, 37(7): 591-598. |
| [6] | Zang Jiajia, Gao Yanfeng, Han Shuzhi, Ping Fen. Acute eosinophilic pneumonia in the elderly: A case report and literature review [J]. Clinical Focus, 2022, 37(10): 931-933. |
| [7] | Ding Hang, Liu Yuan, Zhang Lianfeng, Zhou Lin. Diagnostic value of serum IgG4 for IgG4-related diseases: A meta-analysis [J]. Clinical Focus, 2021, 36(7): 587-594. |
| [8] | Du Zhongcai1, Liu Yu2, Zhou Xinbei2, Zhao Wanjun2, Su Yuan2. A metaanalysis of 30 cases of colchicine poisoning [J]. Clinical Focus, 2020, 35(4): 362-368. |
| [9] | Li Guanhonga, Li Wena, Zeng Jianb, Zhang Yua, Qiu Qingpinga, Zheng Yuqionga. Analysis of clinical characteristics of 12 patients with COVID-19 [J]. Clinical Focus, 2020, 35(11): 1005-1009. |
| [10] | Feng Liancai, Wang Li. Medication in patients with bronchial asthma in Rizhao city [J]. Clinical Focus, 2017, 32(5): 441-443. |
| [11] | Lu Xiaowei, Zhou Hong. Diagnosis and treatment in Graves’ ophthalmopathy [J]. Clinical Focus, 2016, 31(3): 241-245. |
| [12] | CHANG Rong-tian;SHANG De-min;JIANG Jia-yao. Glucocorticoids in treatment of patients with acute respiratory distress syndrome in intensive care unit [J]. Clinical Focus, 2014, 29(6): 685-688. |
| [13] | PENG Jun. Advances in the treatment of refractory/relapsed immune thrombocytopenia [J]. Clinical Focus, 2014, 29(10): 1091-1094. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||