Clinical Focus ›› 2024, Vol. 39 ›› Issue (3): 197-207.doi: 10.3969/j.issn.1004-583X.2024.03.001
Tonsillectomy as a therapy for patients with IgA nephropathy: A meta-analysis
Sun Shuaigang, Zhai Yaling( ), Zhang Wenhui, Tian Huijuan
), Zhang Wenhui, Tian Huijuan
- Department of Nephrology, the First Affiliated Hospital of Zhengzhou University, the Renal Research Institution of Zhengzhou University, Zhengzhou 450052, China
-
Received:2023-03-09Online:2024-03-20Published:2024-06-12 -
Contact:Zhai Yaling E-mail:zhaiyaling1988@163.com
CLC Number:
Cite this article
Sun Shuaigang, Zhai Yaling, Zhang Wenhui, Tian Huijuan. Tonsillectomy as a therapy for patients with IgA nephropathy: A meta-analysis[J]. Clinical Focus, 2024, 39(3): 197-207.
share this article
Add to citation manager EndNote|Ris|BibTeX
URL: https://huicui.hebmu.edu.cn/EN/10.3969/j.issn.1004-583X.2024.03.001
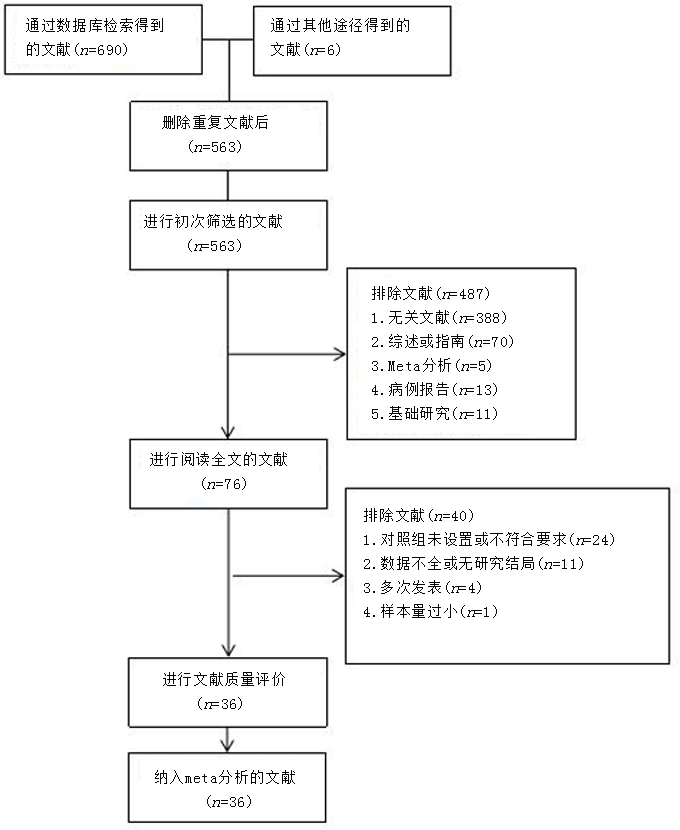
Fig.1 Flow chart of literature screening
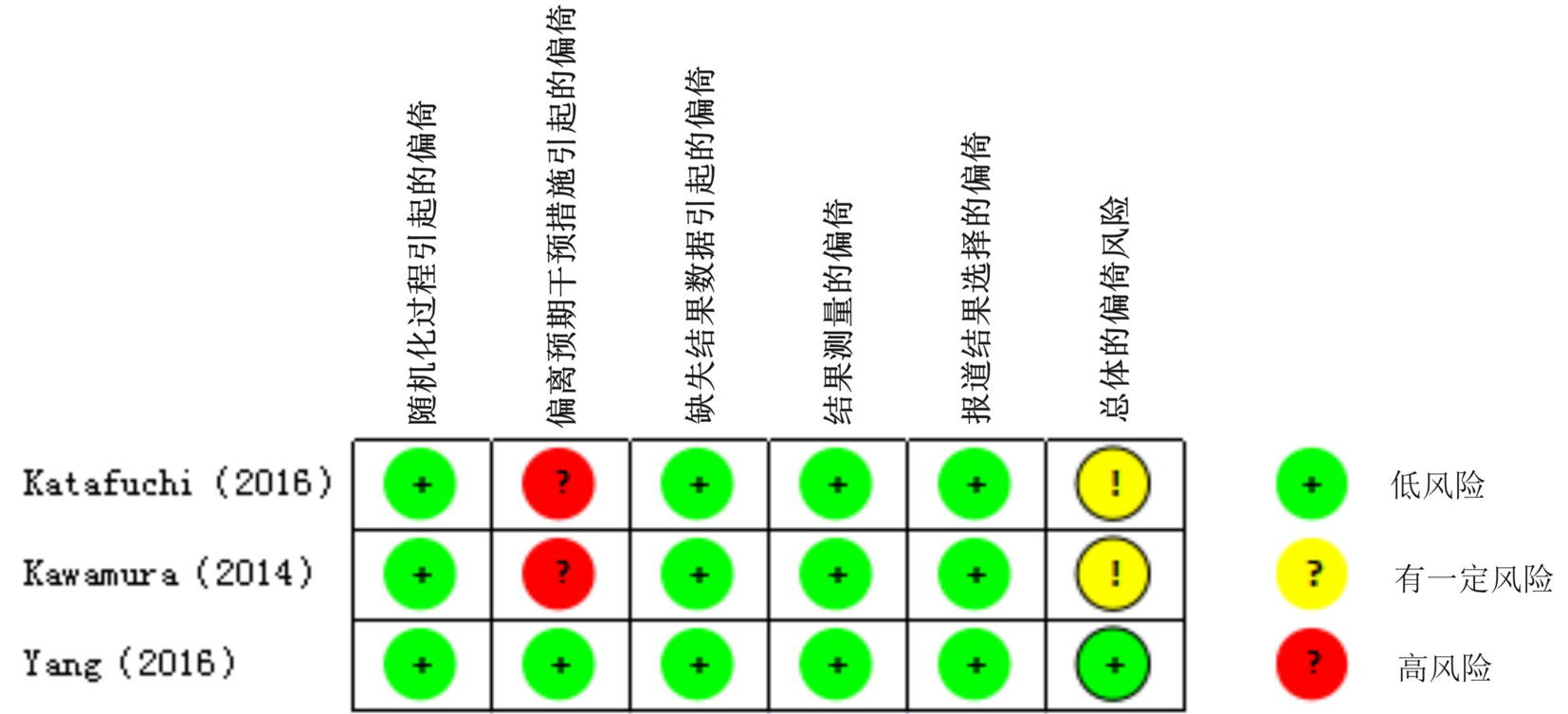
Fig.2 Risk-of-bias assessment in RCT studies
| 作者(年份) | 国家/ 地区 | 研究 类型 | 患者数量 (T/NT) | 年龄 (岁) | 性别 (男/女) | 治疗方式 | 观察结局 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 干预组 | 对照组 | 随访时间 (年) | 尿蛋白 缓解 | 尿红细胞 缓解 | 完全 缓解 | ESRD | NOS | |||||||
| 冯凤仪( | 中国 | PC | 32/34 | 7.4 | 40/26 | T+S | S | 0.5 | - | 22/12 | 7 | |||
| 黄远航( | 中国 | R | 109/98 | 30.7 | 114/93 | T+S | S | 1.0 | - | 89/50 | 7 | |||
| 江枫( | 中国 | PC | 35/40 | - | 38/37 | T | S | 0.5 | - | 16/13 | 2/8 | 7 | ||
| 刘虹( | 中国 | CC | 57/51 | 32.0 | 56/52 | T+S | S | 1.0 | - | 47/22 | 7 | |||
| 孟骏( | 中国 | PC | 24/18 | 31.6 | 16/26 | T+S | S | 1.0 | 19/8 | 18/3 | 15/3 | 7 | ||
| 田滨瑶( | 中国 | R | 34/49 | 32.7 | 42/41 | T/T+S/T+I/T+S+I | S/I/S+I/保守治疗 | 3.9 | - | 17/17 | 7 | |||
| 吴和燕( | 中国 | R | 40/80 | 14.3 | 70/50 | T+S | S | 8.1 | - | 29/36 | 2/4 | 8 | ||
| 肖爱华( | 中国 | PC | 12/15 | 21.4 | 17/10 | T | S | 0.5 | - | 10/2 | 7 | |||
| 于二峰( | 中国 | PC | 59/31 | 30.3 | 34/56 | T+S | S | 3.0 | 47/13 | 49/9 | 7 | |||
| 俞雨生( | 中国 | PC | 41/39 | 25.4 | 59/21 | T | S | 1.5 | - | 19/9 | 7 | |||
| Akagi( | 日本 | RCC | 41/30 | 31.1 | 32/39 | T+S | S | 13.0 | - | 10/4 | 2/8 | 8 | ||
| Chen( | 中国 | RCC | 54/58 | 27.3 | 66/46 | T+S | S | 10.8 | - | 25/16 | 2/7 | 8 | ||
| Feehally( | 意大利 | MRCS | 41/41 | 35.5 | 42/40 | T+S | S | 3.3 | - | 3/8 | 7 | |||
| Hirano( | 日本 | MRCS | 252/813 | 35.0 | 535/530 | T+无S/S/SP | 无S/S/SP | 5.8 | - | 11/118 | 8 | |||
| Hoshino( | 日本 | MCS | 209/918 | 44.1 | 638/489 | T+SP | SP/S/保守治疗 | 8.3 | - | 7/146 | 8 | |||
| Hoshino( | 日本 | RCS | 26/26 | 32.6 | 18/34 | T+SP | S | 6.0 | - | 15/5 | 8 | |||
| Hotta( | 日本 | RCS | 191/34 | 34.4 | - | T+S/SP | S/SP | 6.9 | - | 114/12 | 8 | |||
| Hotta( | 日本 | PC | 26/19 | 30.2 | 17/28 | T+SP | SP | 3.0 | 14/5 | 20/8 | 7 | |||
| Katafuchi( | 日本 | RCT | 26/33 | 39.2 | 27/32 | T+S | S | 4.8 | 16/13 | 18/20 | 12/9 | - | ||
| Kawaguchi( | 日本 | RCS | 307/81 | 34.3 | 177/211 | T+S or T | S | 5.0 | - | 197/19 | 8 | |||
| Kawamura( | 日本 | MRCT | 33/39 | 38.2 | 35/37 | T+S | S | 1.0 | 20/14 | 22/23 | 15/10 | - | ||
| Kawasaki( | 日本 | PC | 16/16 | 12.2 | 17/15 | T+SP | S | 2.0 | - | 12/9 | 7 | |||
| Komatsu( | 日本 | PNC | 35/20 | 34.5 | 21/34 | T+S | S | 4.5 | 23/7 | 27/9 | 19/5 | 0/1 | 7 | |
| Komatsu( | 日本 | MRCS | 46/33 | 34.9 | 31/48 | T+S | S or保守治疗 | 4.7 | 37/15 | 38/18 | 33/14 | 0/1 | 7 | |
| Maeda( | 日本 | RCS | 70/130 | 31.7 | 67/133 | T+S/SP | S+SP | 5.2 | - | 24/12 | 8 | |||
| Matsumoto( | 日本 | RCS | 87/87 | 31.0 | 68/106 | T+S/SP | S+SP | 7.8 | - | 6/22 | 8 | |||
| Miyamoto( | 日本 | MRCS | 161/123 | 37.3 | 123/161 | T+S | S or保守治疗 | 4.1 | - | 92/49 | 7 | |||
| Miyazaki( | 日本 | MPCS | 78/23 | 34.4 | 43/58 | T or T+S | S or保守治疗 | 5.0 | - | 52/10 | 8 | |||
| Nishi( | 日本 | R | 46/74 | 32.6 | 69/51 | T+S | S | 16.4 | - | 5/19 | 8 | |||
| Ochi( | 日本 | RCS | 26/15 | 31.1 | 15/26 | T+S | S | 1.0 | 20/8 | 23/5 | 18/2 | 7 | ||
| Ogura( | 日本 | RCS | 32/80 | 32.0 | 49/63 | T+S | S or保守治疗 | 5.0 | 26/37 | 26/37 | 24/31 | 0/0 | 8 | |
| Ohya( | 日本 | RCS | 41/21 | 34.6 | 20/42 | T+S | S | 5.8 | - | 24/10 | 8 | |||
| Rasche( | 日本 | RCS | 16/39 | 29.0 | 38/17 | T+S | S | 3.4 | - | 10/14 | 7 | |||
| Sato( | 日本 | RCS | 30/40 | 46.5 | 51/19 | T+S | S or保守治疗 | 5.9 | - | 4/25 | 8 | |||
| Xie( | 日本 | RCS | 48/70 | 32.3 | 64/54 | T+S | S | 16.1 | - | 5/18 | 8 | |||
| Yang( | 中国 | RCT | 49/49 | 30.0 | 45/53 | T+S | S | 4.0 | 47/25 | 45/23 | - | |||
Tab.1 Basic characteristics of the eligible studies in this meta-analysis
| 作者(年份) | 国家/ 地区 | 研究 类型 | 患者数量 (T/NT) | 年龄 (岁) | 性别 (男/女) | 治疗方式 | 观察结局 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 干预组 | 对照组 | 随访时间 (年) | 尿蛋白 缓解 | 尿红细胞 缓解 | 完全 缓解 | ESRD | NOS | |||||||
| 冯凤仪( | 中国 | PC | 32/34 | 7.4 | 40/26 | T+S | S | 0.5 | - | 22/12 | 7 | |||
| 黄远航( | 中国 | R | 109/98 | 30.7 | 114/93 | T+S | S | 1.0 | - | 89/50 | 7 | |||
| 江枫( | 中国 | PC | 35/40 | - | 38/37 | T | S | 0.5 | - | 16/13 | 2/8 | 7 | ||
| 刘虹( | 中国 | CC | 57/51 | 32.0 | 56/52 | T+S | S | 1.0 | - | 47/22 | 7 | |||
| 孟骏( | 中国 | PC | 24/18 | 31.6 | 16/26 | T+S | S | 1.0 | 19/8 | 18/3 | 15/3 | 7 | ||
| 田滨瑶( | 中国 | R | 34/49 | 32.7 | 42/41 | T/T+S/T+I/T+S+I | S/I/S+I/保守治疗 | 3.9 | - | 17/17 | 7 | |||
| 吴和燕( | 中国 | R | 40/80 | 14.3 | 70/50 | T+S | S | 8.1 | - | 29/36 | 2/4 | 8 | ||
| 肖爱华( | 中国 | PC | 12/15 | 21.4 | 17/10 | T | S | 0.5 | - | 10/2 | 7 | |||
| 于二峰( | 中国 | PC | 59/31 | 30.3 | 34/56 | T+S | S | 3.0 | 47/13 | 49/9 | 7 | |||
| 俞雨生( | 中国 | PC | 41/39 | 25.4 | 59/21 | T | S | 1.5 | - | 19/9 | 7 | |||
| Akagi( | 日本 | RCC | 41/30 | 31.1 | 32/39 | T+S | S | 13.0 | - | 10/4 | 2/8 | 8 | ||
| Chen( | 中国 | RCC | 54/58 | 27.3 | 66/46 | T+S | S | 10.8 | - | 25/16 | 2/7 | 8 | ||
| Feehally( | 意大利 | MRCS | 41/41 | 35.5 | 42/40 | T+S | S | 3.3 | - | 3/8 | 7 | |||
| Hirano( | 日本 | MRCS | 252/813 | 35.0 | 535/530 | T+无S/S/SP | 无S/S/SP | 5.8 | - | 11/118 | 8 | |||
| Hoshino( | 日本 | MCS | 209/918 | 44.1 | 638/489 | T+SP | SP/S/保守治疗 | 8.3 | - | 7/146 | 8 | |||
| Hoshino( | 日本 | RCS | 26/26 | 32.6 | 18/34 | T+SP | S | 6.0 | - | 15/5 | 8 | |||
| Hotta( | 日本 | RCS | 191/34 | 34.4 | - | T+S/SP | S/SP | 6.9 | - | 114/12 | 8 | |||
| Hotta( | 日本 | PC | 26/19 | 30.2 | 17/28 | T+SP | SP | 3.0 | 14/5 | 20/8 | 7 | |||
| Katafuchi( | 日本 | RCT | 26/33 | 39.2 | 27/32 | T+S | S | 4.8 | 16/13 | 18/20 | 12/9 | - | ||
| Kawaguchi( | 日本 | RCS | 307/81 | 34.3 | 177/211 | T+S or T | S | 5.0 | - | 197/19 | 8 | |||
| Kawamura( | 日本 | MRCT | 33/39 | 38.2 | 35/37 | T+S | S | 1.0 | 20/14 | 22/23 | 15/10 | - | ||
| Kawasaki( | 日本 | PC | 16/16 | 12.2 | 17/15 | T+SP | S | 2.0 | - | 12/9 | 7 | |||
| Komatsu( | 日本 | PNC | 35/20 | 34.5 | 21/34 | T+S | S | 4.5 | 23/7 | 27/9 | 19/5 | 0/1 | 7 | |
| Komatsu( | 日本 | MRCS | 46/33 | 34.9 | 31/48 | T+S | S or保守治疗 | 4.7 | 37/15 | 38/18 | 33/14 | 0/1 | 7 | |
| Maeda( | 日本 | RCS | 70/130 | 31.7 | 67/133 | T+S/SP | S+SP | 5.2 | - | 24/12 | 8 | |||
| Matsumoto( | 日本 | RCS | 87/87 | 31.0 | 68/106 | T+S/SP | S+SP | 7.8 | - | 6/22 | 8 | |||
| Miyamoto( | 日本 | MRCS | 161/123 | 37.3 | 123/161 | T+S | S or保守治疗 | 4.1 | - | 92/49 | 7 | |||
| Miyazaki( | 日本 | MPCS | 78/23 | 34.4 | 43/58 | T or T+S | S or保守治疗 | 5.0 | - | 52/10 | 8 | |||
| Nishi( | 日本 | R | 46/74 | 32.6 | 69/51 | T+S | S | 16.4 | - | 5/19 | 8 | |||
| Ochi( | 日本 | RCS | 26/15 | 31.1 | 15/26 | T+S | S | 1.0 | 20/8 | 23/5 | 18/2 | 7 | ||
| Ogura( | 日本 | RCS | 32/80 | 32.0 | 49/63 | T+S | S or保守治疗 | 5.0 | 26/37 | 26/37 | 24/31 | 0/0 | 8 | |
| Ohya( | 日本 | RCS | 41/21 | 34.6 | 20/42 | T+S | S | 5.8 | - | 24/10 | 8 | |||
| Rasche( | 日本 | RCS | 16/39 | 29.0 | 38/17 | T+S | S | 3.4 | - | 10/14 | 7 | |||
| Sato( | 日本 | RCS | 30/40 | 46.5 | 51/19 | T+S | S or保守治疗 | 5.9 | - | 4/25 | 8 | |||
| Xie( | 日本 | RCS | 48/70 | 32.3 | 64/54 | T+S | S | 16.1 | - | 5/18 | 8 | |||
| Yang( | 中国 | RCT | 49/49 | 30.0 | 45/53 | T+S | S | 4.0 | 47/25 | 45/23 | - | |||
| 作者(年份) | 选择 | 基于设计或分析的 队列的可比性 | 结局 | 总分 | |||||
|---|---|---|---|---|---|---|---|---|---|
| 暴露队列 的代表性 | 非暴露队 列的选择 | 暴露的 确定 | 研究开始前没有研究 对象出现结局事件 | 结局事件 的评估 | 为观察到结局事件, 随访是否充分 | 随访的 完整性 | |||
| 冯凤仪( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 黄远航( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 江枫( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 刘虹( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 孟骏( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 田滨瑶( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 吴和燕( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| 肖爱华( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 于二峰( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 俞雨生( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Akagi( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Chen( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Feehally( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Hirano( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Hoshino( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Hoshino( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Hotta( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Hotta( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Kawaguchi( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Kawasaki( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Komatsu( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Komatsu( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Maeda( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Matsumoto( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Miyamoto( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Miyazaki( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Nishi( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Ochi( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Ogura( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Ohya( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Rasche( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Sato( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Xie( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
Tab.2 Quality assessment of the eligible cohort studies according to the Newcastle-Ottawa Scale (NOS)
| 作者(年份) | 选择 | 基于设计或分析的 队列的可比性 | 结局 | 总分 | |||||
|---|---|---|---|---|---|---|---|---|---|
| 暴露队列 的代表性 | 非暴露队 列的选择 | 暴露的 确定 | 研究开始前没有研究 对象出现结局事件 | 结局事件 的评估 | 为观察到结局事件, 随访是否充分 | 随访的 完整性 | |||
| 冯凤仪( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 黄远航( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 江枫( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 刘虹( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 孟骏( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 田滨瑶( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 吴和燕( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| 肖爱华( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 于二峰( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| 俞雨生( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Akagi( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Chen( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Feehally( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Hirano( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Hoshino( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Hoshino( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Hotta( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Hotta( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Kawaguchi( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Kawasaki( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Komatsu( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Komatsu( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Maeda( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Matsumoto( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Miyamoto( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Miyazaki( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Nishi( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Ochi( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Ogura( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Ohya( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Rasche( | ★ | ★ | ★ | ★ | ★★ | ★ | ☆ | ☆ | 7 |
| Sato( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| Xie( | ★ | ★ | ★ | ★ | ★★ | ★ | ★ | ☆ | 8 |
| 研究 | 研究目的 是否明确 | 纳入患者 完整性 | 预期数据 收集 | 终点指标反应 研究目的 | 终点指标 评价 | 随访 时间 | 失访率 | 样本量 估算 | 对照组 选择 | 对照组 同步性 | 组间基线 可比 | 统计 分析 | 质量评价 得分 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Komatsu( | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 22 |
Tab.3 Entries for methodological index for non-randomized studies (MINORS)
| 研究 | 研究目的 是否明确 | 纳入患者 完整性 | 预期数据 收集 | 终点指标反应 研究目的 | 终点指标 评价 | 随访 时间 | 失访率 | 样本量 估算 | 对照组 选择 | 对照组 同步性 | 组间基线 可比 | 统计 分析 | 质量评价 得分 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Komatsu( | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 22 |
| 作者(年份) | 蛋白尿缓解 | 血尿缓解 | 临床缓解 | ESRD |
|---|---|---|---|---|
| 冯凤仪( | - | - | 术后半年肉眼血尿消失,1 h尿沉渣红细胞计数、24 h尿蛋白定量恢复正常 | - |
| 黄远航( | - | - | 尿蛋白定量持续<0.15 g/24 h,尿红细胞<8000/ml | - |
| 江枫( | - | - | 肾功能正常,半年以上血尿、蛋白尿阴性 | 终末期肾衰竭行透析或肾移植治疗 |
| 刘虹( | - | - | 尿红细胞<8000/ml,尿蛋白24 h持续<0.15 g | - |
| 孟骏( | 尿蛋白消失 | 尿潜血消失 | 尿蛋白或尿潜血消失 | - |
| 田滨瑶( | - | - | 尿蛋白转阴,24 h尿蛋白定量<0.3 g/d,血清白蛋白(ALB)>35 g/L,肾功能不全者血肌酐(sCr)下降或稳定 | - |
| 吴和燕( | - | - | 肾功能正常,蛋白尿和血尿阴性(尿蛋白量<0.4 g/24 h,尿红细胞<104/ml),且随访期间无复发 | 初始估算肾小球滤过率(eGFR)<15 ml·min-1/1.73 m2或需要接受肾脏替代治疗 |
| 肖爱华( | - | - | 24 h尿蛋白定量、1 h尿红细胞计数恢复正常 | - |
| 于二峰( | 尿蛋白较基础值下降 ≤0.3 g/d | 尿红细胞较基础值减少 ≤2.0万/ml | - | - |
| 俞雨生( | - | - | 肉眼血尿消失,尿化验阴性,血浆蛋白及肾功能正常,临床症状体征消失 | - |
| Akagi( | - | - | 肾功能正常,无蛋白尿和血尿 | 需要透析的患者 |
| Chen( | - | - | 随访期间肾功能正常,蛋白尿和血尿呈阴性(尿蛋白排泄量<0.4 g/d,尿红细胞<10000个/ml),无复发 | sCr水平超过8 mg/dl(707 μmol/L)或进行透析或肾移植 |
| Feehally( | - | - | - | eGFR降低50%或终末期肾病 |
| Hirano( | - | - | - | 首次出现sCr从基线或透析开始增加1.5倍 |
| Hoshino( | - | - | - | 开始透析治疗 |
| Hoshino( | - | - | 在6个月内观察到3次24h蛋白尿<0.3 g/gCr或0.3 g/d,尿红细胞<5/HPF | - |
| Hotta( | - | - | 尿蛋白和血尿阴性,尿红细胞为4/高倍视野或更低 | - |
| Hotta( | 持续3个月蛋白尿<100 mg/d | 持续3个月<3红细胞/HP | - | |
| Katafuchi( | 尿蛋白排泄量<0.3 g/d,或<0.3 g/g Cr | 尿沉渣中的红细胞数量<5/HPF | 蛋白尿和血尿消失 | - |
| Kawaguchi( | - | - | 尿蛋白完全消失,尿红细胞小于1/高倍视野 | - |
| Kawamura( | 蛋白尿消失 | 血尿消失 | 蛋白尿和(或)血尿消失 | - |
| Kawasaki( | - | - | 尿液和肾功能正常 | - |
| Komatsu( | 蛋白尿消失 | 血尿消失 | 蛋白尿和(或)血尿消失 | sCr比基线水平增加100% |
| Komatsu( | 至少连续2次24 h尿蛋白<0.3 g/d,尿蛋白/尿肌酐比值<0.3或尿蛋白定性(-)~(±) | 至少连续两次在尿沉渣镜检<5/HPF或浸棒试验中红细胞(-)~(±) | 血尿和蛋白尿消失 | 肾功能下降50%,sCr较基线升高100%,或肾脏替代治疗 |
| Maeda( | - | - | 至少相隔3个月连续2次就诊时血尿和蛋白尿正常 | - |
| Matsumoto( | - | - | - | |
| Miyamoto( | - | - | 至少连续2次蛋白尿和血尿的缓解:蛋白尿为阴性或微量或尿蛋白排泄量<0.3 g/g Cr;尿沉渣中的红细胞数量<5/HPF | - |
| Miyazaki( | - | - | - | - |
| Nishi( | - | - | - | 开始透析治疗 |
| Ochi( | 24 h蛋白尿<0.3 g/g Cr | 尿红细胞<5/HPF | 24 h蛋白尿<0.3 g/g Cr和尿红细胞<5/HPF | - |
| Ogura( | 连续3次发现24 h蛋白尿<0.3 g/g Cr或尿蛋白定性(-)或(±) | 连续3次发现红细胞<5/HPF或定性测量(-)或(±) | 血尿和蛋白尿缓解 | 开始透析治疗 |
| Ohya( | - | - | 尿蛋白或尿潜血消失 | - |
| Rasche( | - | - | - | 开始透析治疗 |
| Sato( | - | - | - | 开始透析治疗 |
| Xie( | - | - | - | 开始透析治疗 |
| Yang( | 尿蛋白<0.3 g/d | 尿沉渣中的红细胞<5/HPF | 蛋白尿和血尿消失 | - |
Tab.4 Definitions for proteinuria remission, hematuria remission, clinical remission, and ESRD in relevant studies
| 作者(年份) | 蛋白尿缓解 | 血尿缓解 | 临床缓解 | ESRD |
|---|---|---|---|---|
| 冯凤仪( | - | - | 术后半年肉眼血尿消失,1 h尿沉渣红细胞计数、24 h尿蛋白定量恢复正常 | - |
| 黄远航( | - | - | 尿蛋白定量持续<0.15 g/24 h,尿红细胞<8000/ml | - |
| 江枫( | - | - | 肾功能正常,半年以上血尿、蛋白尿阴性 | 终末期肾衰竭行透析或肾移植治疗 |
| 刘虹( | - | - | 尿红细胞<8000/ml,尿蛋白24 h持续<0.15 g | - |
| 孟骏( | 尿蛋白消失 | 尿潜血消失 | 尿蛋白或尿潜血消失 | - |
| 田滨瑶( | - | - | 尿蛋白转阴,24 h尿蛋白定量<0.3 g/d,血清白蛋白(ALB)>35 g/L,肾功能不全者血肌酐(sCr)下降或稳定 | - |
| 吴和燕( | - | - | 肾功能正常,蛋白尿和血尿阴性(尿蛋白量<0.4 g/24 h,尿红细胞<104/ml),且随访期间无复发 | 初始估算肾小球滤过率(eGFR)<15 ml·min-1/1.73 m2或需要接受肾脏替代治疗 |
| 肖爱华( | - | - | 24 h尿蛋白定量、1 h尿红细胞计数恢复正常 | - |
| 于二峰( | 尿蛋白较基础值下降 ≤0.3 g/d | 尿红细胞较基础值减少 ≤2.0万/ml | - | - |
| 俞雨生( | - | - | 肉眼血尿消失,尿化验阴性,血浆蛋白及肾功能正常,临床症状体征消失 | - |
| Akagi( | - | - | 肾功能正常,无蛋白尿和血尿 | 需要透析的患者 |
| Chen( | - | - | 随访期间肾功能正常,蛋白尿和血尿呈阴性(尿蛋白排泄量<0.4 g/d,尿红细胞<10000个/ml),无复发 | sCr水平超过8 mg/dl(707 μmol/L)或进行透析或肾移植 |
| Feehally( | - | - | - | eGFR降低50%或终末期肾病 |
| Hirano( | - | - | - | 首次出现sCr从基线或透析开始增加1.5倍 |
| Hoshino( | - | - | - | 开始透析治疗 |
| Hoshino( | - | - | 在6个月内观察到3次24h蛋白尿<0.3 g/gCr或0.3 g/d,尿红细胞<5/HPF | - |
| Hotta( | - | - | 尿蛋白和血尿阴性,尿红细胞为4/高倍视野或更低 | - |
| Hotta( | 持续3个月蛋白尿<100 mg/d | 持续3个月<3红细胞/HP | - | |
| Katafuchi( | 尿蛋白排泄量<0.3 g/d,或<0.3 g/g Cr | 尿沉渣中的红细胞数量<5/HPF | 蛋白尿和血尿消失 | - |
| Kawaguchi( | - | - | 尿蛋白完全消失,尿红细胞小于1/高倍视野 | - |
| Kawamura( | 蛋白尿消失 | 血尿消失 | 蛋白尿和(或)血尿消失 | - |
| Kawasaki( | - | - | 尿液和肾功能正常 | - |
| Komatsu( | 蛋白尿消失 | 血尿消失 | 蛋白尿和(或)血尿消失 | sCr比基线水平增加100% |
| Komatsu( | 至少连续2次24 h尿蛋白<0.3 g/d,尿蛋白/尿肌酐比值<0.3或尿蛋白定性(-)~(±) | 至少连续两次在尿沉渣镜检<5/HPF或浸棒试验中红细胞(-)~(±) | 血尿和蛋白尿消失 | 肾功能下降50%,sCr较基线升高100%,或肾脏替代治疗 |
| Maeda( | - | - | 至少相隔3个月连续2次就诊时血尿和蛋白尿正常 | - |
| Matsumoto( | - | - | - | |
| Miyamoto( | - | - | 至少连续2次蛋白尿和血尿的缓解:蛋白尿为阴性或微量或尿蛋白排泄量<0.3 g/g Cr;尿沉渣中的红细胞数量<5/HPF | - |
| Miyazaki( | - | - | - | - |
| Nishi( | - | - | - | 开始透析治疗 |
| Ochi( | 24 h蛋白尿<0.3 g/g Cr | 尿红细胞<5/HPF | 24 h蛋白尿<0.3 g/g Cr和尿红细胞<5/HPF | - |
| Ogura( | 连续3次发现24 h蛋白尿<0.3 g/g Cr或尿蛋白定性(-)或(±) | 连续3次发现红细胞<5/HPF或定性测量(-)或(±) | 血尿和蛋白尿缓解 | 开始透析治疗 |
| Ohya( | - | - | 尿蛋白或尿潜血消失 | - |
| Rasche( | - | - | - | 开始透析治疗 |
| Sato( | - | - | - | 开始透析治疗 |
| Xie( | - | - | - | 开始透析治疗 |
| Yang( | 尿蛋白<0.3 g/d | 尿沉渣中的红细胞<5/HPF | 蛋白尿和血尿消失 | - |
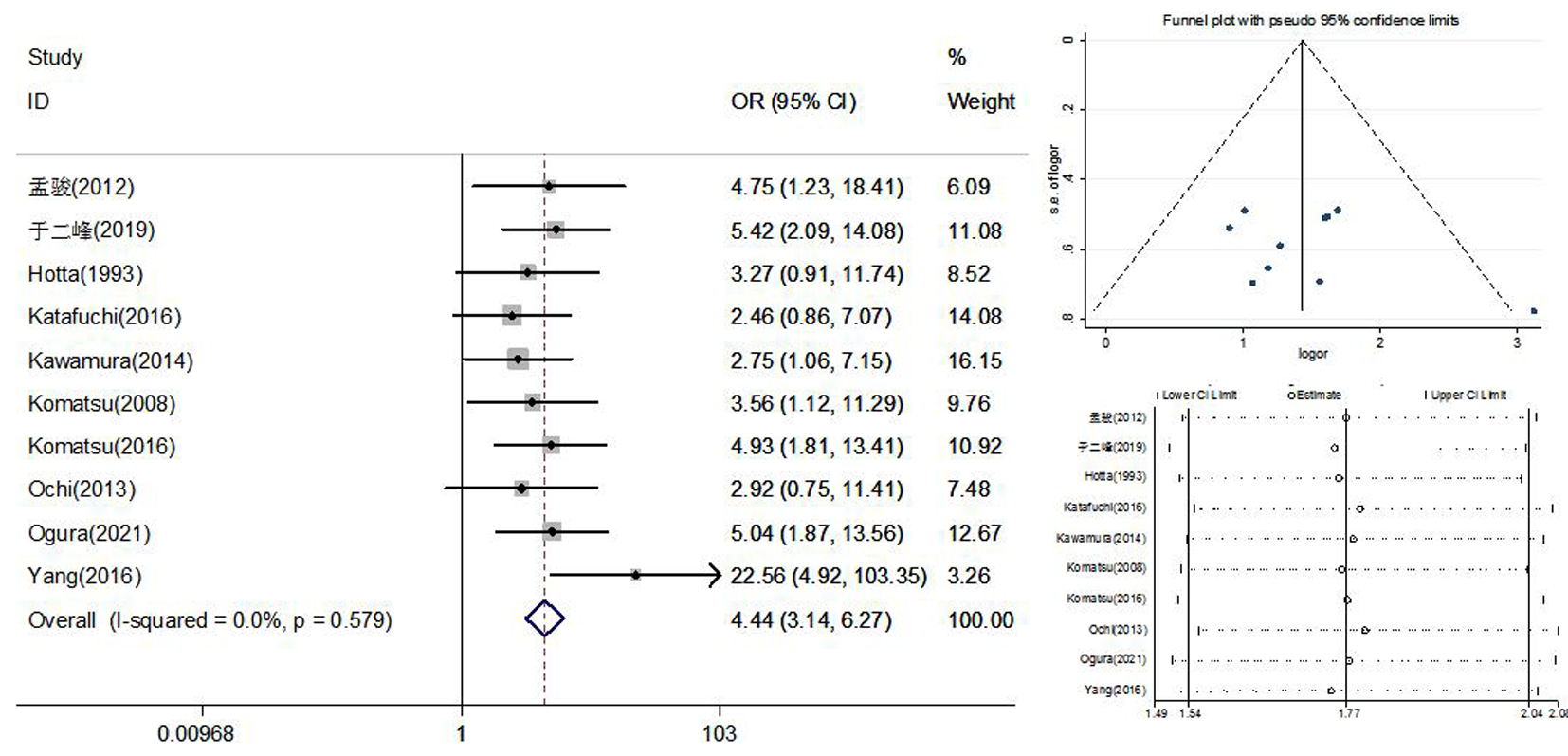
Fig. 3 Meta-analysis of proteinuria remission rate after IgAN treatment with tonsillectomy
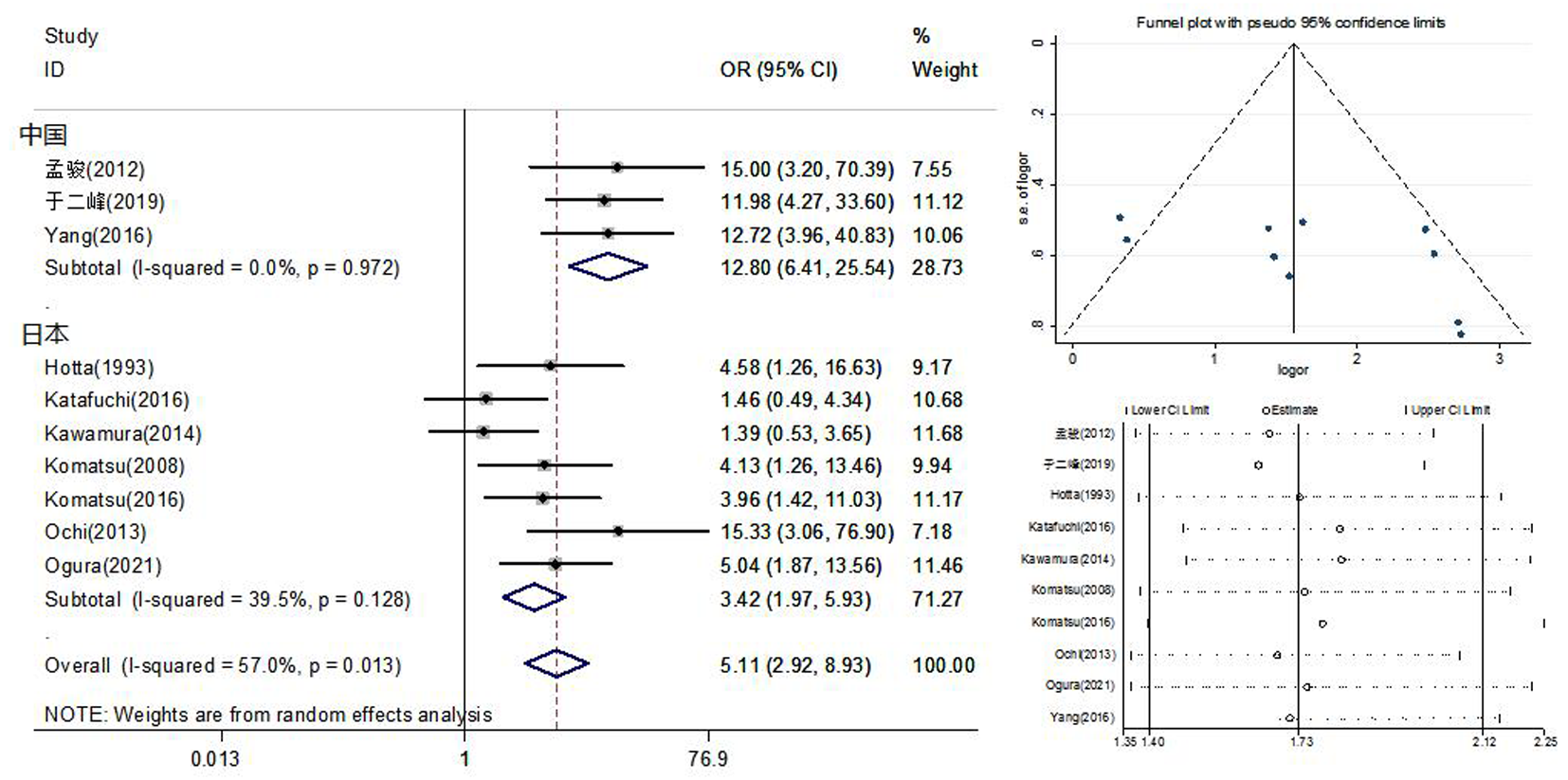
Fig. 4 Meta-analysis and subgroup analysis of hematuria remission rate after IgAN treatment by tonsillectomy
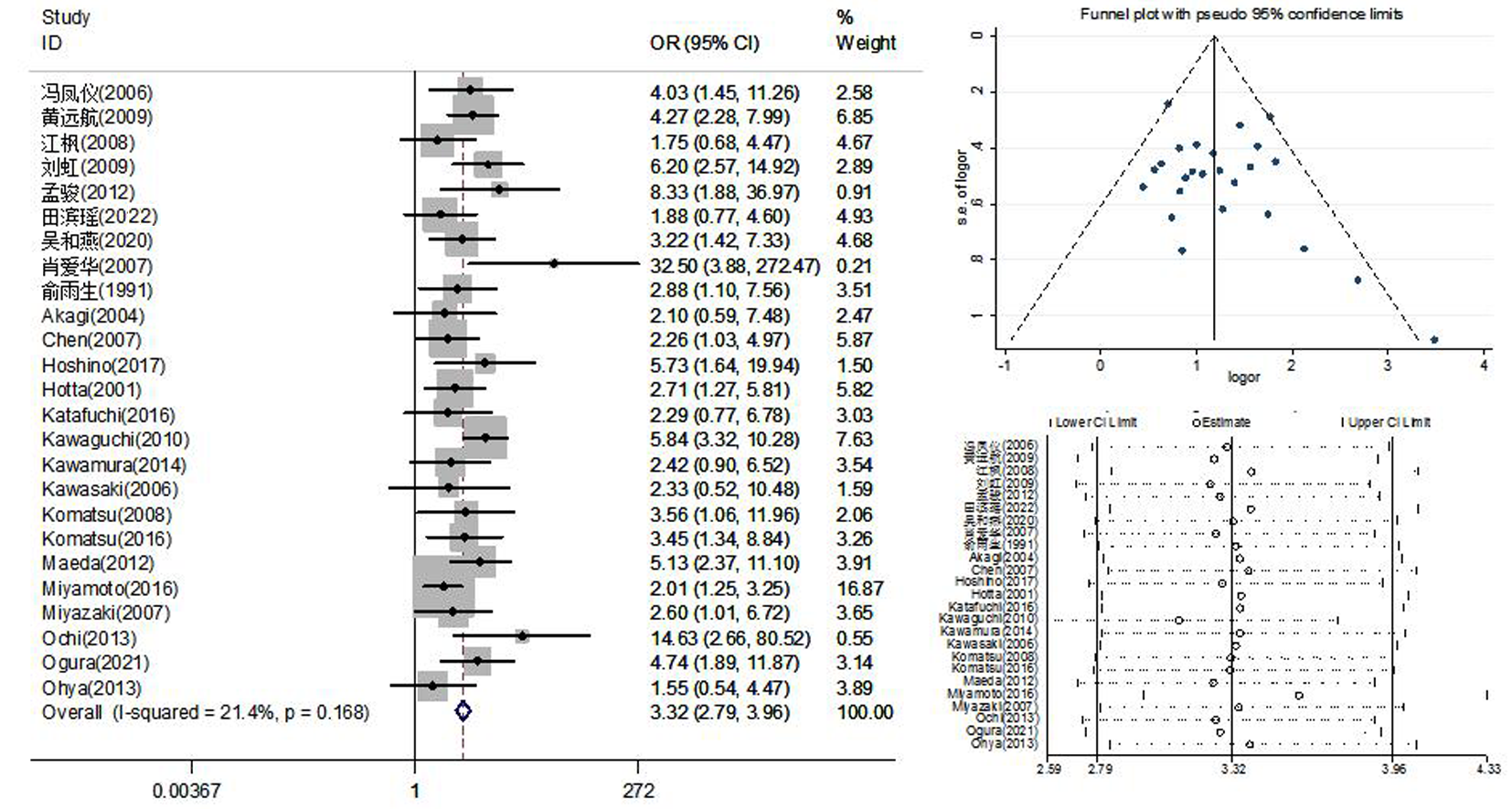
Fig. 5 Meta-analysis of CR rate after IgAN treatment by tonsillectomy
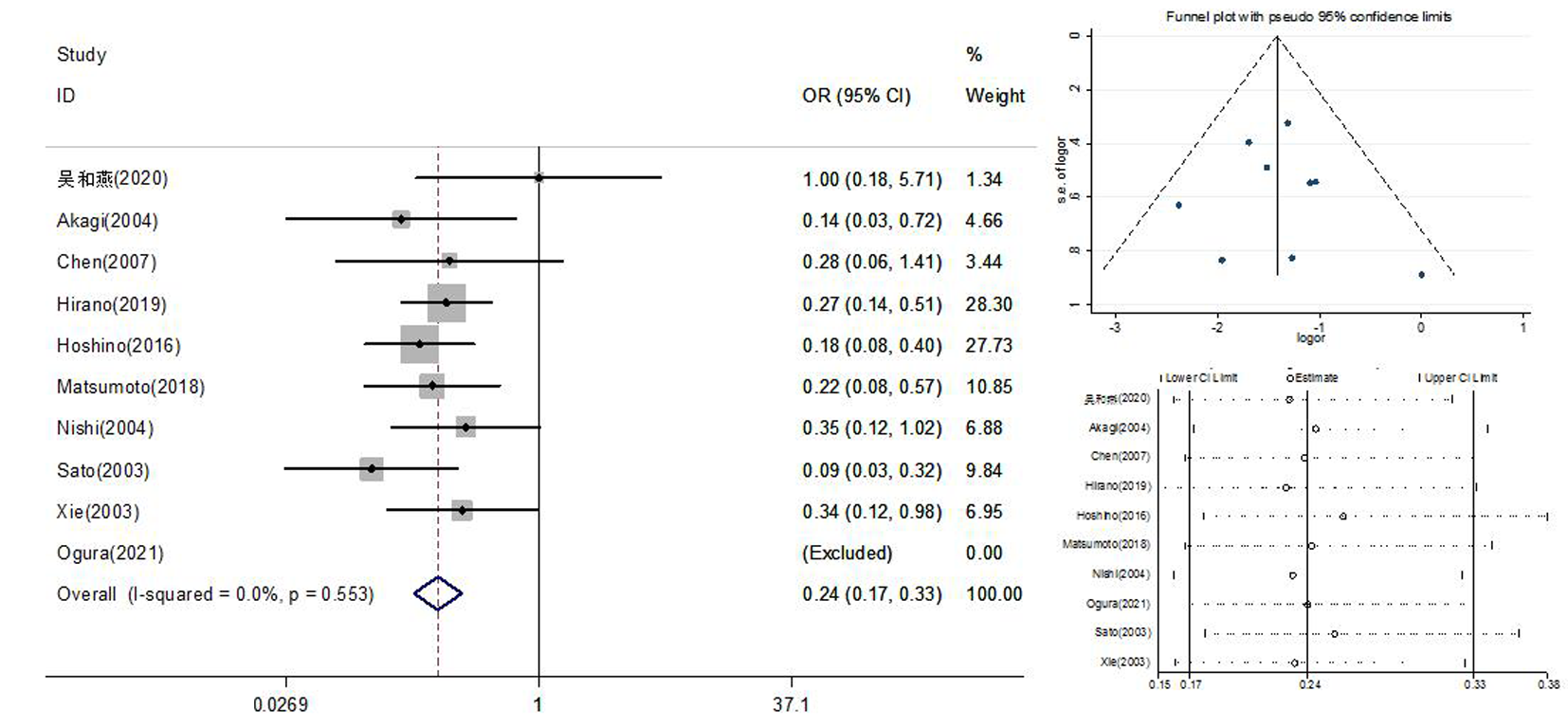
Fig. 6 Meta-analysis of the incidence of ESRD after IgAN treatment by tonsillectomy and subgroup analysis based on the follow-up duration
| [1] |
D'Amico G. Natural history of idiopathic IgA nephropathy and factors predictive of disease outcome[J]. Semin Nephrol, 2004, 24(3):179-196.
doi: 10.1016/j.semnephrol.2004.01.001 pmid: 15156525 |
| [2] |
Sugiyama H, Yokoyama H, Sato H, et al. Japan Renal Biopsy Registry: The first nationwide, web-based, and prospective registry system of renal biopsies in Japan[J]. Clin Exp Nephrol, 2011, 15(4):493-503.
doi: 10.1007/s10157-011-0430-4 pmid: 21437579 |
| [3] | Wyatt RJ, Julian BA. IgA nephropathy[J]. N Engl J Med, 2013, 368(25):2402-2414. |
| [4] |
Koyama A, Igarashi M, Kobayashi M. Natural history and risk factors for immunoglobulin A nephropathy in Japan. Research Group on Progressive Renal Diseases[J]. Am J Kidney Dis, 1997, 29(4):526-532.
pmid: 9100040 |
| [5] |
Lai KN, Tang SC, Schena FP, et al. IgA nephropathy[J]. Nat Rev Dis Primers, 2016, 2:16001.
doi: 10.1038/nrdp.2016.1 pmid: 27189177 |
| [6] |
D'Amico G. Idiopathic IgA mesangial nephropathy[J]. Nephron, 1985, 41(1):1-13.
pmid: 3897881 |
| [7] | Geddes CC, Rauta V, Gronhagen-Riska C, et al. A tricontinental view of IgA nephropathy[J]. Nephrol Dial Transplant, 2003, 18(8):1541-1548. |
| [8] |
Appel GB, Waldman M. The IgA nephropathy treatment dilemma[J]. Kidney Int, 2006, 69(11):1939-1944.
pmid: 16641925 |
| [9] |
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses[J]. Eur J Epidemiol, 2010, 25(9):603-605.
doi: 10.1007/s10654-010-9491-z pmid: 20652370 |
| [10] |
Slim K, Nini E, Forestier D, et al. Methodological index for non-randomized studies (minors): Development and validation of a new instrument[J]. ANZ J Surg, 2003, 73(9): 712-716.
doi: 10.1046/j.1445-2197.2003.02748.x pmid: 12956787 |
| [11] | Higgins JPT, Savovi'c J, Page MJ, et al. Chapter 8: Assessing risk of bias in a randomized trial. In: Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023) Cochrane, 2023. Available from: www.training.cochrane.org/handbook. |
| [12] | 冯凤仪, 邓燕, 李超雄, 等. 扁桃体切除治疗儿童 IgA 肾病的疗效观察[J]. 中国医师杂志, 2006, 8(9):1242, 1245. |
| [13] | 黄远航, 范立明, 童俊容, 等. 半量激素联合霉酚酸酯治疗扁桃体摘除术后IgA肾病的疗效观察[J]. 中国药房, 2009, 20(26):2043-2044. |
| [14] | 江枫. 扁桃体切除术对IgA肾病的治疗及预后因素预测[J]. 中国医师进修杂志, 2008, 31(21):28-30. |
| [15] | 刘虹, 彭佑铭, 刘伏友, 等. 扁桃体摘除治疗57例IgA肾病的病例对照研究[J]. 中华肾脏病杂志, 2009, 25(1):64-65. |
| [16] | 孟骏. 扁桃体切除术联合激素对IgA肾病的疗效评价[J]. 安徽医学, 2012, 33(9):1160-1163. |
| [17] | 田滨瑶, 周俊蕾, 李悦, 等. 扁桃体切除术对合并慢性扁桃体炎的IgA肾病患者预后的影响[J]. 中国实用内科杂志, 2022, 42(8):655-659. |
| [18] |
吴和燕, 高春林, 彭映潮, 等. 扁桃体切除联合糖皮质激素治疗对IgA肾病患儿长期临床缓解和肾脏预后的影响[J]. 中华肾脏病杂志, 2020, 36(10):766-772.
doi: 10.3760/cma.j.cn441217-20191203-00135 |
| [19] | 肖爱华. 慢性扁桃体炎合并IgA肾病临床观察[J]. 中国误诊学杂志, 2007, 7(22):5257-5258. |
| [20] | 于二峰, 高明, 杨亚茹, 等. 腭扁桃体摘除联合雷公藤多甙与强的松治疗IgA肾病远期疗效随访[J]. 临床心身疾病杂志, 2019, 25(1):94-96, 121. |
| [21] | 俞雨生, 黎磊石, 王庆文, 等. 扁桃体切除治疗以肉眼血尿为主的IgA肾病[J]. 中华医学杂志, 1991, 71(4):226-228. |
| [22] | Akagi H, Kosaka M, Hattori K, et al. Long-term results of tonsillectomy as a treatment for IgA nephropathy[J]. Acta Otolaryngol Suppl, 2004, (555):38-42. |
| [23] |
Chen Y, Tang Z, Wang Q, et al. Long-term efficacy of tonsillectomy in Chinese patients with IgA nephropathy[J]. Am J Nephrol, 2007, 27(2):170-175.
doi: 10.1159/000100431 pmid: 17337885 |
| [24] | Feehally J, Coppo R, Troyanov S, et al. Tonsillectomy in a European cohort of 1, 147 patients with IgA nephropathy[J]. Nephron, 2016, 132(1):15-24. |
| [25] | Hirano K, Matsuzaki K, Yasuda T, et al. Association between tonsillectomy and outcomes in patients with immunoglobulin A nephropathy[J]. JAMA Netw Open, 2019, 2(5):e194772. |
| [26] |
Hoshino J, Fujii T, Usui J, et al. Renal outcome after tonsillectomy plus corticosteroid pulse therapy in patients with immunoglobulin A nephropathy: Results of a multicenter cohort study[J]. Clin Exp Nephrol, 2016, 20(4):618-627.
doi: 10.1007/s10157-015-1194-z pmid: 26577676 |
| [27] |
Hoshino Y, Moriyama T, Uchida K, et al. Comparison of oral steroids with tonsillectomy plus steroid pulse therapy in patients with IgA nephropathy[J]. Clin Exp Nephrol, 2017, 21(4):617-623.
doi: 10.1007/s10157-016-1324-2 pmid: 27549901 |
| [28] |
Hotta O, Miyazaki M, Furuta T, et al. Tonsillectomy and steroid pulse therapy significantly impact on clinical remission in patients with IgA nephropathy[J]. Am J Kidney Dis, 2001, 38(4):736-743.
doi: 10.1053/ajkd.2001.27690 pmid: 11576876 |
| [29] | Hotta O, Taguma Y, Kurosawa K, et al. Early intensive therapy for clinical remission of active IgA nephropathy: A three-year follow-up study[J]. Nihon Jinzo Gakkai Shi, 1993, 35(8):967-973. |
| [30] |
Katafuchi R, Kawamura T, Joh K, et al. Pathological sub-analysis of a multicenter randomized controlled trial of tonsillectomy combined with steroid pulse therapy versus steroid pulse monotherapy in patients with immunoglobulin A nephropathy[J]. Clin Exp Nephrol, 2016, 20(2):244-252.
doi: 10.1007/s10157-015-1159-2 pmid: 26349433 |
| [31] | Kawaguchi T, Ieiri N, Yamazaki S, et al. Clinical effectiveness of steroid pulse therapy combined with tonsillectomy in patients with immunoglobulin A nephropathy presenting glomerular haematuria and minimal proteinuria[J]. Nephrology (Carlton), 2010, 15(1):116-123. |
| [32] | Kawamura T, Yoshimura M, Miyazaki Y, et al. A multicenter randomized controlled trial of tonsillectomy combined with steroid pulse therapy in patients with immunoglobulin A nephropathy[J]. Nephrol Dial Transplant, 2014, 29(8):1546-1553. |
| [33] |
Kawasaki Y, Takano K, Suyama K, et al. Efficacy of tonsillectomy pulse therapy versus multiple-drug therapy for IgA nephropathy[J]. Pediatr Nephrol, 2006, 21(11):1701-1706.
pmid: 16932894 |
| [34] | Komatsu H, Fujimoto S, Hara S, et al. Effect of tonsillectomy plus steroid pulse therapy on clinical remission of IgA nephropathy: A controlled study[J]. Clin J Am Soc Nephrol, 2008, 3(5):1301-1317. |
| [35] |
Komatsu H, Sato Y, Miyamoto T, et al. Significance of tonsillectomy combined with steroid pulse therapy for IgA nephropathy with mild proteinuria[J]. Clin Exp Nephrol, 2016, 20(1):94-102.
doi: 10.1007/s10157-015-1138-7 pmid: 26123429 |
| [36] | Maeda I, Hayashi T, Sato KK, et al. Tonsillectomy has beneficial effects on remission and progression of IgA nephropathy independent of steroid therapy[J]. Nephrol Dial Transplant, 2012, 27(7):2806-2813. |
| [37] | Matsumoto K, Ikeda Y, Yamaguchi S, et al. Long-term outcomes of tonsillectomy for IgA nephropathy patients: A retrospective cohort study, two-centre analysis with the inverse probability therapy weighting method[J]. Nephrology (Carlton), 2018, 23(9):846-854. |
| [38] |
Miyamoto T, Nishino T, Nakata T, et al. Impact of tonsillectomy combined with steroid pulse therapy on immunoglobulin A nephropathy depending on histological classification: A multicenter study[J]. Clin Exp Nephrol, 2016, 20(1):50-57.
doi: 10.1007/s10157-015-1131-1 pmid: 26055039 |
| [39] |
Miyazaki M, Hotta O, Komatsuda A, et al. A multicenter prospective cohort study of tonsillectomy and steroid therapy in Japanese patients with IgA nephropathy: A 5-year report[J]. Contrib Nephrol, 2007, 157:94-98.
pmid: 17495443 |
| [40] | Nishi S, Xie Y, Ueno M, et al. A clinicopathological study on the long-term efficacy of tonsillectomy in patients with IgA nephropathy[J]. Acta Otolaryngol Suppl, 2004, (555):49-53. |
| [41] |
Ochi A, Moriyama T, Takei T, et al. Comparison between steroid pulse therapy alone and in combination with tonsillectomy for IgA nephropathy[J]. Int Urol Nephrol, 2013, 45(2):469-476.
doi: 10.1007/s11255-012-0251-8 pmid: 22833253 |
| [42] |
Ogura S, Moriyama T, Miyabe Y, et al. Evaluation of appropriate treatment for IgA nephropathy with mild proteinuria and normal renal function[J]. Clin Exp Nephrol, 2021, 25(10):1103-1110.
doi: 10.1007/s10157-021-02086-9 pmid: 34101029 |
| [43] |
Ohya M, Otani H, Minami Y, et al. Tonsillectomy with steroid pulse therapy has more effect on the relapse rate than steroid pulse monotherapy in IgA nephropathy patients[J]. Clin Nephrol, 2013, 80(1):47-52.
doi: 10.5414/CN107861 pmid: 23557791 |
| [44] |
Rasche FM, Schwarz A, Keller F. Tonsillectomy does not prevent a progressive course in IgA nephropathy[J]. Clin Nephrol, 1999, 51(3):147-152.
pmid: 10099887 |
| [45] |
Sato M, Hotta O, Tomioka S, et al. Cohort study of advanced IgA nephropathy: Efficacy and limitations of corticosteroids with tonsillectomy[J]. Nephron Clin Pract, 2003, 93(4):c137-145.
doi: 10.1159/000070233 pmid: 12759582 |
| [46] |
Xie Y, Nishi S, Ueno M, et al. The efficacy of tonsillectomy on long-term renal survival in patients with IgA nephropathy[J]. Kidney Int, 2003, 63(5):1861-1867.
pmid: 12675864 |
| [47] |
Yang D, He L, Peng X, et al. The efficacy of tonsillectomy on clinical remission and relapse in patients with IgA nephropathy: A randomized controlled trial[J]. Ren Fail, 2016, 38(2):242-248.
doi: 10.3109/0886022X.2015.1128251 pmid: 26727697 |
| [48] |
Hotta O. Use of corticosteroids, other immunosuppressive therapies, and tonsillectomy in the treatment of IgA nephropathy[J]. Semin Nephrol, 2004, 24(3):244-255.
pmid: 15156529 |
| [49] |
Rovin BH, Adler SG, Barratt J, et al. Executive summary of the KDIGO 2021 guideline for the management of glomerular diseases[J]. Kidney Int, 2021, 100(4):753-779.
doi: 10.1016/j.kint.2021.05.015 pmid: 34556300 |
| Viewed | ||||||||||||||||||||||||||||||||||||||||||||||||||
|
Full text 28
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
Abstract 163
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||